

The Difference Between Cystatin C- and Creatinine-Based Estimated GFR and Associations With Frailty and Adverse Outcomes: A Cohort Analysis of the Systolic Blood Pressure Intervention Trial (SPRINT)
- PMID: 32682697
- PMCID: PMC8896529
- DOI: 10.1053/j.ajkd.2020.05.017
The Difference Between Cystatin C- and Creatinine-Based Estimated GFR and Associations With Frailty and Adverse Outcomes: A Cohort Analysis of the Systolic Blood Pressure Intervention Trial (SPRINT)
Abstract
Rationale & objective: In prior research and in practice, the difference between estimated glomerular filtration rate (eGFR) calculated from cystatin C level and eGFR calculated from creatinine level has not been assessed for clinical significance and relevance. We evaluated whether these differences contain important information about frailty.
Study design: A cohort analysis of the Systolic Blood Pressure Intervention Trial (SPRINT).
Setting & participants: 9,092 hypertensive SPRINT participants who had baseline measurements of serum creatinine, cystatin C, and frailty.
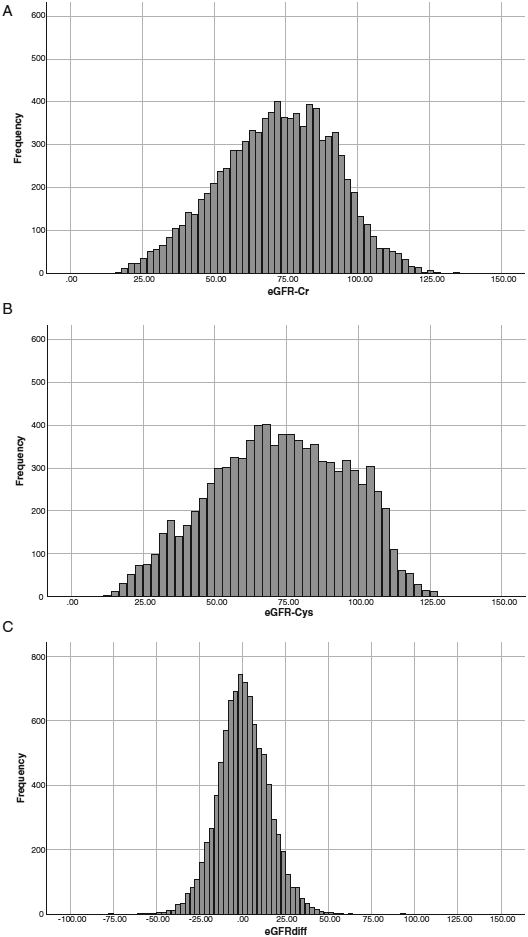
Exposure: eGFRs calculated using CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) equations (eGFRcys and eGFRcr), and eGFRDiff, calculated as eGFRcys-eGFRcr.
Outcomes: A validated 35-item frailty index that included questionnaire data for general and physical health, limitations of activities, pain, depression, sleep, energy level, self-care, and smoking status, as well as medical history, cognitive assessment, and laboratory data. We defined frailty as frailty index score>0.21 (range, 0-1). The incidence of injurious falls, hospitalizations, cardiovascular events, and mortality was also recorded.
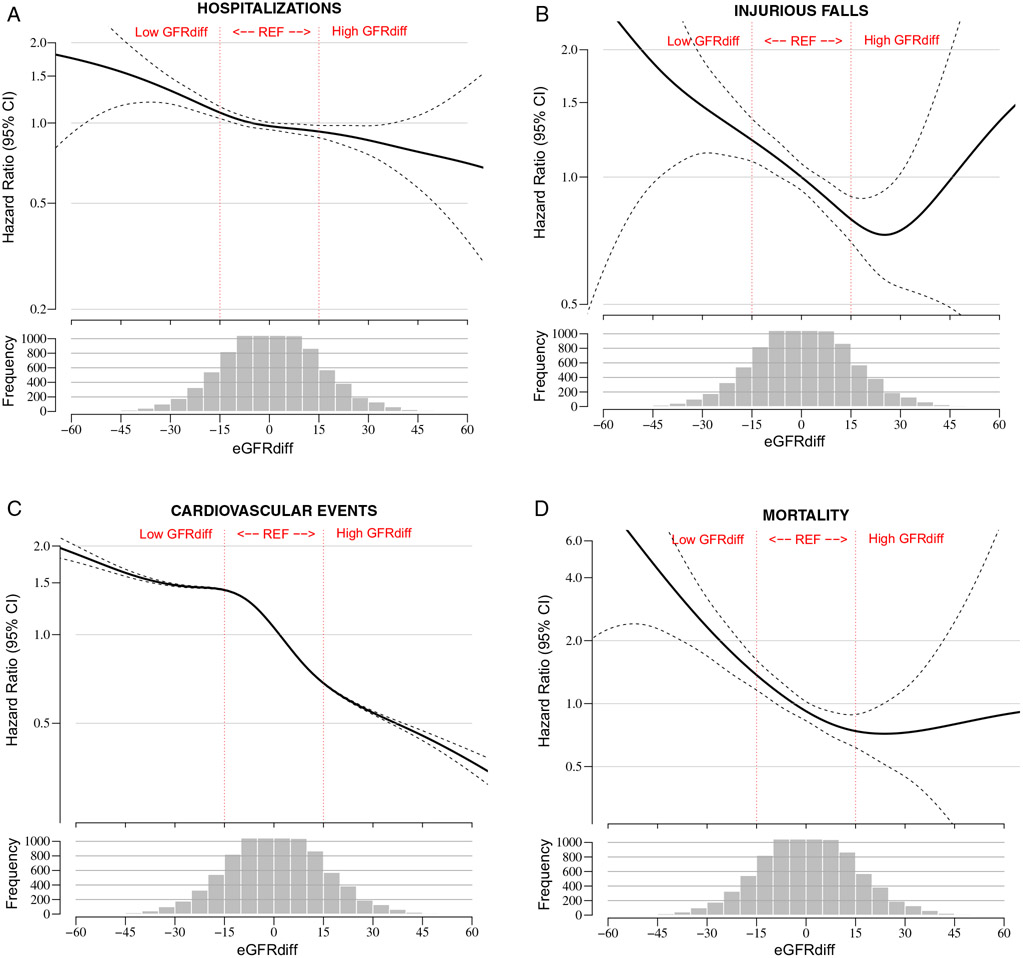
Analytical approach: We used logistic regression to model the cross-sectional association of baseline eGFRDiff with frailty among all SPRINT participants. Adjusted proportional hazards regression was used to evaluate the association of eGFRDiff with adverse outcomes and mortality.
Results: Mean age was 68±9 (SD) years, mean eGFRcys and eGFRcr were 73±23 and 72±20mL/min/1.73m2, and mean eGFRDiff was 0.5±15mL/min/1.73m2. In adjusted models, each 1-SD higher eGFRDiff was associated with 24% lower odds of prevalent frailty (OR, 0.76; 95% CI, 0.71-0.81), as well as with lower incidence rate of injurious falls (HR, 0.84; 95% CI, 0.77-0.92), hospitalization (HR, 0.91; 95% CI, 0.88-0.95), cardiovascular events (HR, 0.89; 95% CI, 0.81-0.97), and all-cause mortality (HR, 0.71; 95% CI, 0.63-0.82); P<0.01.
Limitations: Gold-standard measure of kidney function and assessment of muscle mass were not available.
Conclusions: The difference between eGFRcys and eGFRcr is associated with frailty and health status. Positive eGFRDiff is strongly associated with lower risks for longitudinal adverse outcomes and mortality, even after adjusting for chronic kidney disease stage and baseline frailty.
Keywords: Estimated glomerular filtration rate (eGFR); aging; cardiovascular disease; cystatin C; death; falls; filtration marker; frailty; kidney function; muscle mass; older adults; renal disease; risk stratification; sarcopenia; serum creatinine.
Copyright © 2020 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Differences Between Cystatin C- and Creatinine-Based Estimated GFR-Early Evidence of a Clinical Marker for Frailty.Am J Kidney Dis. 2020 Dec;76(6):752-753. doi: 10.1053/j.ajkd.2020.07.010. Epub 2020 Oct 7. Am J Kidney Dis. 2020. PMID: 33039174 Free PMC article. No abstract available.
References
-
- Rule AD, Lieske JC. Cystatin C is more than GFR, and this may be a good thing. J Am Soc Nephrol. 2011;22(5):795–797. - PubMed
-
- Coll E, Botey A, Alvarez L, et al. Serum cystatin C as a new marker for noninvasive estimation of glomerular filtration rate and as a marker for early renal impairment. Am J Kidney Dis. 2000;36(1):29–34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 TR000433/TR/NCATS NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- R01 DK098234/DK/NIDDK NIH HHS/United States
- UL1 TR000064/TR/NCATS NIH HHS/United States
- UL1 TR000075/TR/NCATS NIH HHS/United States
- UL1 TR000093/TR/NCATS NIH HHS/United States
- T32 DK104717/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000050/TR/NCATS NIH HHS/United States
- UL1 RR025755/RR/NCRR NIH HHS/United States
- K24 DK110427/DK/NIDDK NIH HHS/United States
- K23 DK091521/DK/NIDDK NIH HHS/United States
- P30 AG021332/AG/NIA NIH HHS/United States
- HHSN268200900048C/HL/NHLBI NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- HHSN268200900040C/HL/NHLBI NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- HHSN268200900046C/HL/NHLBI NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- UL1 TR001064/TR/NCATS NIH HHS/United States
- UL1 RR025752/RR/NCRR NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
- HHSN268200900049C/HL/NHLBI NIH HHS/United States
- HHSN268200900047C/HL/NHLBI NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 TR000073/TR/NCATS NIH HHS/United States
- UL1 TR000002/TR/NCATS NIH HHS/United States
- UL1 TR000105/TR/NCATS NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
- UL1 TR003142/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
