

Evidence-Based Practices for Acute Respiratory Failure and Acute Respiratory Distress Syndrome: A Systematic Review of Reviews
- PMID: 32682771
- PMCID: PMC7768938
- DOI: 10.1016/j.chest.2020.06.080
Evidence-Based Practices for Acute Respiratory Failure and Acute Respiratory Distress Syndrome: A Systematic Review of Reviews
Abstract
Background: The recent pandemic highlights the essential nature of optimizing the use of invasive mechanical ventilation (IMV) in complex critical care settings. This review of reviews maps evidence-based practices (EBPs) that are associated with better outcomes among adult patients with acute respiratory failure or ARDS on the continuum of care, from intubation to liberation.
Research question: What EPBs are recommended to reduce the duration of IMV and mortality rate among patients with acute respiratory failure/ARDS?
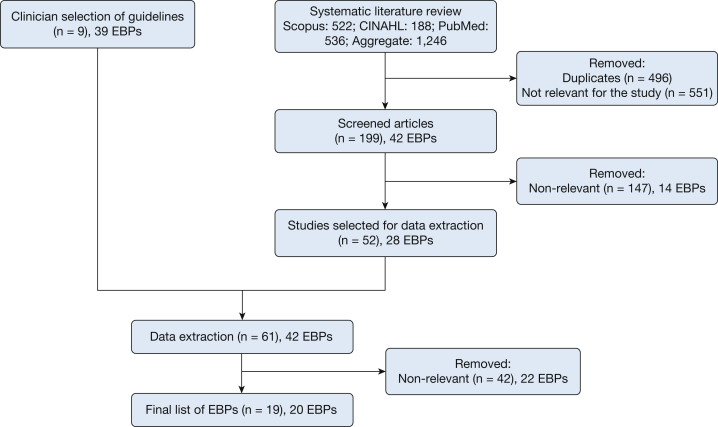
Study design and methods: We identified an initial set of reports that links EBPs to mortality rates and/or duration of IMV. We conducted a review of reviews, focusing on preappraised guidelines, meta-analyses, and systematic reviews. We searched Scopus, CINAHL, and PubMed from January 2016 to January 2019 for additional evidence that has not yet been incorporated into current guidelines.
Results: Our initial search produced 61 publications that contained 42 EBPs. We excluded 42 manuscripts during the data extraction process, primarily because they were not associated with improved patient outcomes. The remaining 19 preappraised guidelines, meta-analyses, and systematic reviews met our full inclusion criteria and spanned the continuum of IMV care from intubation to liberation. These contained 20 EBPs, a majority of which were supported with moderate levels of evidence. Of these, six EBPs focused on intubation and escalation of care, such as ventilator management and synchrony; ten EBPs reduced complications associated with IMV, which included spontaneous awakening and breathing trials and early mobility protocols; and four EBPs promoted timely extubation and postextubation recovery.
Interpretation: This review describes EBPs that are associated with fewer ventilator days and/or lower mortality rates among patients who received IMV for acute respiratory failure/ARDS. Many of these EBPs are connected across the care continuum, which indicates the need to promote and assess effective implementation jointly, rather than individually.
Keywords: ARDS; acute respiratory failure; evidence-based practice; invasive mechanical ventilation.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Wunsch H., Linde-Zwirble W.T., Angus D.C., Hartman M.E., Milbrandt E.B., Kahn J.M. The epidemiology of mechanical ventilation use in the United States. Criti Care Med. 2010;38(10):1947–1953. - PubMed
-
- Rubenfeld G.D., Caldwell E., Peabody E. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353(16):1685–1693. - PubMed
-
- Fan E., Del Sorbo L., Goligher E.C. An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;195(9):1253–1263. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
