

The Day after Tomorrow: How Should We Address Health System Organization to Treat Cancer Patients after the Peak of the COVID-19 Epidemic?
- PMID: 32683373
- PMCID: PMC7445382
- DOI: 10.1159/000509650
The Day after Tomorrow: How Should We Address Health System Organization to Treat Cancer Patients after the Peak of the COVID-19 Epidemic?
Abstract
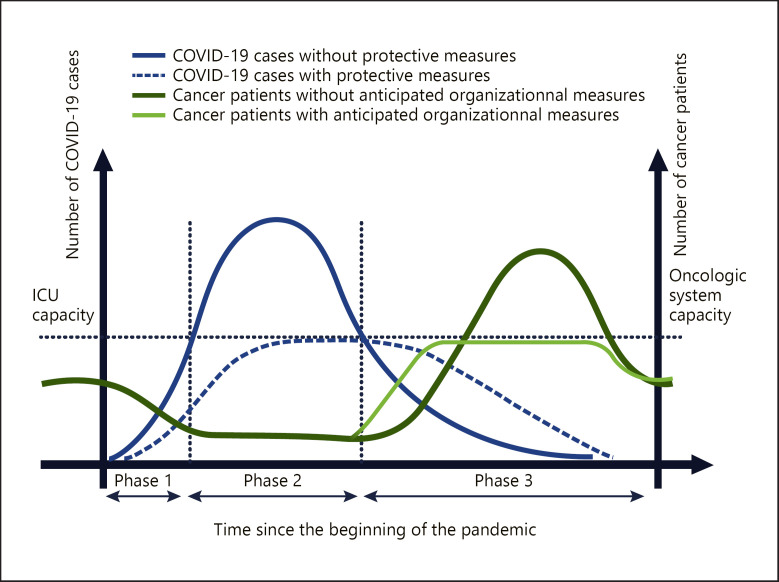
On March 11, 2020, the WHO director general declared COVID-19 a pandemic. This pandemic evolves in successive phases, i.e., phase 1 (the start phase), phase 2 ("the storm"), and phase 3 (the recession). To date, oncology and surgery groups have only given instructions for addressing phases 1 and 2. To prevent excess cancer mortality, health care systems (HCS) need to be restructured. Our aim is to detail the specificities of each epidemic phase and discuss several methods of organization to optimize cancer patient flow during the COVID-19 pandemic, particularly during phase 3. Hospitals must be reorganized in order to create a cancer hub that is free of infection, allowing for the safe treatment of patients. Hospital structures are different, but all allow for the creation of virus-free areas. Screening programs are critical and need to be applied to all people entering the virus-free zone, including health care workers. Some reorganization proposals are internal to a hospital, while others require interhospital collaboration. The heterogeneity and complexity of HCS will make interhospital management difficult. The ministry of health has an important role in managing the cancer crisis. Cancer management should be declared a priority. Oncological and surgical societies must coordinate their efforts to facilitate this prioritization. The anticipation of oncological management during phase 3 of the pandemic is necessary because it requires a complete readjustment of HCS. This adaptation should allow for the continuation of cancer care to prevent excess cancer mortality, as the virus will still be present for a currently undetermined period of time.
Keywords: COVID-19 outbreak; Cancer; Health care systems; Oncology; Pandemic.
© 2020 S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflict of interests to declare.
Figures

Similar articles
-
A Reminder of Skin Cancer During the COVID-19 Pandemic.Acta Dermatovenerol Croat. 2021 Apr;291(1):58. Acta Dermatovenerol Croat. 2021. PMID: 34477068
-
COVID-19 on the Nile: Review on the Management and Outcomes of the COVID-19 Pandemic in the Arab Republic of Egypt from February to August 2020.Int J Environ Res Public Health. 2021 Feb 8;18(4):1588. doi: 10.3390/ijerph18041588. Int J Environ Res Public Health. 2021. PMID: 33567519 Free PMC article. Review.
-
Evaluation of medical practices in oncology in the context of the COVID-19 pandemic in France: Physicians' point of view: the PRATICOVID study.Cancer Med. 2020 Dec;9(23):8875-8883. doi: 10.1002/cam4.3503. Epub 2020 Oct 6. Cancer Med. 2020. PMID: 33022134 Free PMC article.
-
Protective measures for patients with advanced cancer during the Sars-CoV-2 pandemic: Quo vadis?Clin Exp Metastasis. 2021 Jun;38(3):257-261. doi: 10.1007/s10585-021-10083-1. Epub 2021 Mar 23. Clin Exp Metastasis. 2021. PMID: 33759009 Free PMC article.
-
Managing cancer care during the COVID-19 pandemic: brief report from a North African single center.Pan Afr Med J. 2020 Jul 29;35(Suppl 2):127. doi: 10.11604/pamj.supp.2020.35.25020. eCollection 2020. Pan Afr Med J. 2020. PMID: 33282082 Free PMC article.
Cited by
-
[RE: Strategy for the practice of digestive and oncologic surgery in COVID-19 epidemic situation].J Chir Visc. 2021 Feb;158(1):101-102. doi: 10.1016/j.jchirv.2020.11.001. Epub 2020 Nov 20. J Chir Visc. 2021. PMID: 33250944 Free PMC article. French. No abstract available.
-
The Impact of COVID-19 on Cancer Care in the Post Pandemic World: Five Major Lessons Learnt from Challenges and Countermeasures of Major Asian Cancer Centres.Asian Pac J Cancer Prev. 2021 Mar 1;22(3):681-690. doi: 10.31557/APJCP.2021.22.3.681. Asian Pac J Cancer Prev. 2021. PMID: 33773529 Free PMC article.
-
Differences in the Clinical Severity Scores of Hospitalized COVID-19 Patients across Different Phases of an Epidemic Wave in Iran: a Secondary Analysis.Med J Islam Repub Iran. 2024 Aug 13;38:93. doi: 10.47176/mjiri.38.93. eCollection 2024. Med J Islam Repub Iran. 2024. PMID: 39678761 Free PMC article.
-
Cancer Australia consensus statement on COVID-19 and cancer care: embedding high value changes in practice.Med J Aust. 2021 Nov 15;215(10):479-484. doi: 10.5694/mja2.51304. Epub 2021 Oct 24. Med J Aust. 2021. PMID: 34689343 Free PMC article.
-
Impact of preoperative COVID infection on the outcomes of planned curative-intent cancer surgeries in the second wave of the pandemic from a tertiary care center in India.J Surg Oncol. 2022 Feb;125(2):107-112. doi: 10.1002/jso.26697. Epub 2021 Sep 27. J Surg Oncol. 2022. PMID: 34569620 Free PMC article.
References
-
- European Commission . Estimates of cancer incidence and mortality in 2018. Brussels: European Commission; 2020.
-
- American College of Surgeons . COVID-19: recommendations for management of elective surgical procedures. 2020. Available from: https://www.facs.org/covid-19/clinical-guidance/elective-surgery.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
