

Goblet cell carcinoid of the rectum: a case report
- PMID: 32683504
- PMCID: PMC7368876
- DOI: 10.1186/s40792-020-00937-3
Goblet cell carcinoid of the rectum: a case report
Abstract
Background: Goblet cell carcinoid (GCC) is a neuroendocrine tumor usually found in the appendix. GCCs exhibit characteristic findings with mixed endocrine-exocrine features such as staining positive for neuroendocrine markers and producing mucin. The primary GCC of the rectum is exceedingly rare.
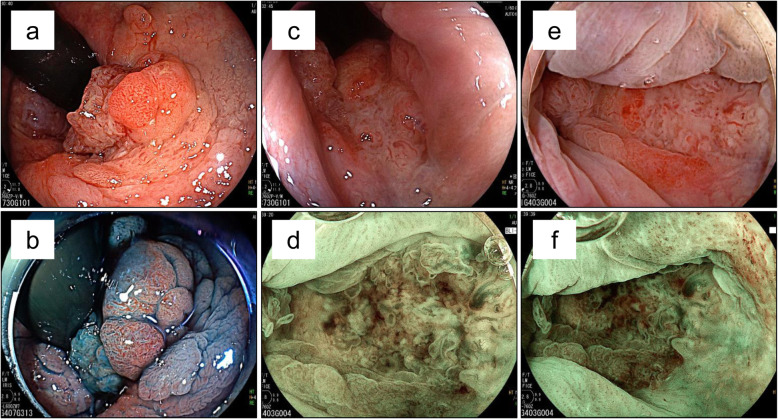
Case presentation: A 77-year-old Japanese male presented with hematochezia. Anal tenderness and a hard mass in the anal canal were found on the digital rectal examination, and colonoscopy was performed. Colonoscopy showed an irregularly shaped mass in the anal canal. Biopsy showed mixed features including adenocarcinoma in situ, well-differentiated adenocarcinoma, and mucinous carcinoma with invasive proliferation. No metastatic lesions were found on the computed tomography scan. Pelvic magnetic resonance imaging scan showed extramural growth of a tumor on the ventral side of the rectum without invasion to the prostate. Laparoscopic abdominoperineal resection was performed. The final diagnosis was well-differentiated adenocarcinoma in the mucosa and goblet cell carcinoid from the submucosa to the adventitia of the rectum. The patient was discharged from the hospital on postoperative day 16. Six months after resection, a computed tomography scan revealed multiple metastatic lesions in the liver. Several chemotherapy regimens were given, and the patient has stable disease 27 months after surgery.
Conclusion: We present a patient with rectal GCC with metachronous liver metastases. Since GCC grows intramurally and is biologically aggressive compared to typical carcinoid lesions, the disease is usually diagnosed at an advanced stage. The development of optimal adjuvant chemotherapy is needed for those patients.
Keywords: Goblet cell carcinoid; Liver metastases; Rectum.
Conflict of interest statement
All authors declare no conflicts of interest regarding the publication of this paper.
Figures






Similar articles
-
Goblet cell carcinoid of the rectum with lymph node metastasis: report of a case.Surg Today. 2011 Sep;41(9):1284-9. doi: 10.1007/s00595-010-4474-y. Epub 2011 Aug 26. Surg Today. 2011. PMID: 21874432
-
Peritoneal metastatic goblet-cell carcinoid tumor treated with cytoreductive surgery and intraperitoneal chemotherapy.Ann Coloproctol. 2015 Apr;31(2):74-8. doi: 10.3393/ac.2015.31.2.74. Epub 2015 Apr 30. Ann Coloproctol. 2015. PMID: 25960976 Free PMC article.
-
Goblet cell carcinoid of the appendix - diagnostic challenges and treatment updates: a case report and review of the literature.J Med Case Rep. 2018 Sep 24;12(1):275. doi: 10.1186/s13256-018-1789-6. J Med Case Rep. 2018. PMID: 30244681 Free PMC article. Review.
-
Combined classical carcinoid and goblet cell carcinoid tumor: a new morphologic variant of carcinoid tumor of the appendix.Am J Surg Pathol. 2010 Aug;34(8):1163-7. doi: 10.1097/PAS.0b013e3181e52916. Am J Surg Pathol. 2010. PMID: 20631606
-
[Carcinoid of the Appendix Goblet Cells Metastasize to the Orbit - a Clinical Case Report and Review of the Literature].Klin Onkol. 2016;29(3):220-3. doi: 10.14735/amko2016220. Klin Onkol. 2016. PMID: 27296408 Review. Czech.
Cited by
-
LSD1 and Aberrant DNA Methylation Mediate Persistence of Enteroendocrine Progenitors That Support BRAF-Mutant Colorectal Cancer.Cancer Res. 2021 Jul 15;81(14):3791-3805. doi: 10.1158/0008-5472.CAN-20-3562. Epub 2021 May 25. Cancer Res. 2021. PMID: 34035083 Free PMC article.
-
A rare goblet cell adenocarcinoma arising from Barrett's esophagus: the first reported case in the esophagus.J Pathol Transl Med. 2024 Mar;58(2):81-86. doi: 10.4132/jptm.2023.12.26. Epub 2024 Jan 8. J Pathol Transl Med. 2024. PMID: 38178706 Free PMC article.
-
Case report: Coexistence of rectal signet ring cell carcinoma with neuroendocrine components.BMC Geriatr. 2025 May 28;25(1):382. doi: 10.1186/s12877-025-06037-x. BMC Geriatr. 2025. PMID: 40437380 Free PMC article.
References
-
- Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, et al. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2008;26(18):3063–3072. doi: 10.1200/JCO.2007.15.4377. - DOI - PubMed
-
- Ueno A, Yokota M, Terada K, Hashida K, Nagahisa Y, Yamaguchi K, et al. Appendiceal goblet cell carcinoid successfully treated with bevacizumab plus mFOLFOX6 regimen-A case report. Gan to kagaku ryoho Cancer & chemotherapy. 2020;47(5):839–842. - PubMed
LinkOut - more resources
Full Text Sources
