

Extent of pulmonary thromboembolic disease in patients with COVID-19 on CT: relationship with pulmonary parenchymal disease
- PMID: 32684301
- PMCID: PMC7351373
- DOI: 10.1016/j.crad.2020.07.002
Extent of pulmonary thromboembolic disease in patients with COVID-19 on CT: relationship with pulmonary parenchymal disease
Abstract
Aim: To report the severity and extent of pulmonary thromboembolic disease (PTD) in COVID-19 patients undergoing computed tomography pulmonary angiography (CTPA) in a tertiary centre.
Materials and methods: This is a retrospective analysis of COVID-19 patients undergoing CTPA over a period of 27 days. The presence, extent, and severity of PTD were documented. Two observers scored the pattern and extent of lung parenchymal disease including potential fibrotic features, as well as lymph node enlargement and pleural effusions. Consensus was achieved via a third observer. Interobserver agreement was assessed using kappa statistics. Student's t-test, chi-squared, and Mann-Whitney U-tests were used to compare imaging features between PTD and non-PTD sub-groups.
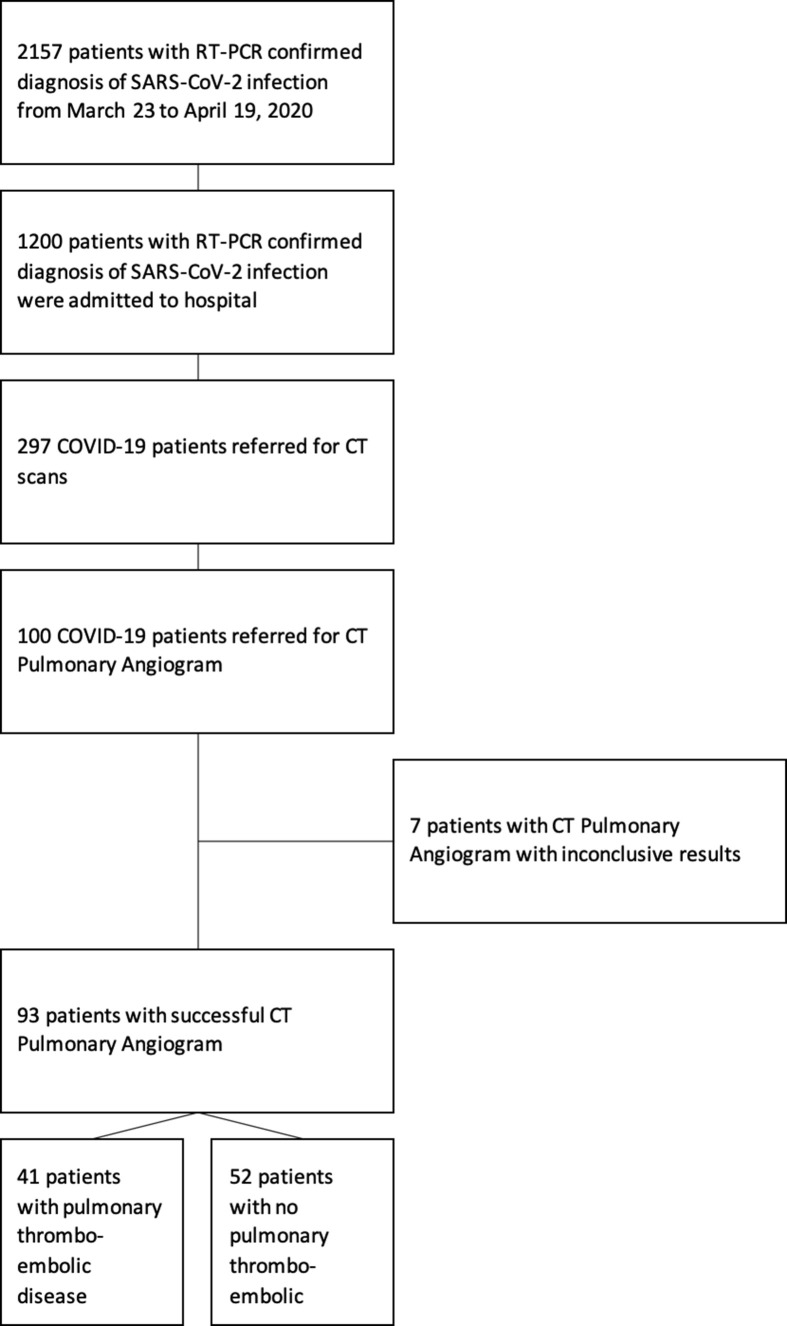
Results: During the study period, 100 patients with confirmed COVID-19 underwent CTPA imaging. Ninety-three studies were analysed, excluding indeterminate CTPA examinations. Overall incidence of PTD was 41/93 (44%) with 28/93 patients showing small vessel PTD (30%). D-dimer was elevated in 90/93 (96.8%) cases. A high Wells' score did not differentiate between PTD and non-PTD groups (p=0.801). The interobserver agreement was fair (kappa=0.659) for parenchymal patterns and excellent (kappa=0.816) for severity. Thirty-four of the 93 cases (36.6%) had lymph node enlargement; 29/34 (85.3%) showed no additional source of infection. Sixteen of the 93 (17.2%) cases had potential fibrotic features.
Conclusion: There is a high incidence of PTD in COVID-19 patients undergoing CTPA and lack of a risk stratification tool. The present data indicates a higher suspicion of PTD is needed in severe COVID-19 patients. The concomitant presence of possible fibrotic features on CT indicates the need for follow-up.
Crown Copyright © 2020. Published by Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Re: extent of pulmonary thromboembolic disease in patients with COVID-19 on CT: relationship with pulmonary parenchymal disease.Clin Radiol. 2020 Dec;75(12):957-959. doi: 10.1016/j.crad.2020.09.019. Epub 2020 Oct 8. Clin Radiol. 2020. PMID: 33077157 Free PMC article. No abstract available.
References
-
- European Centre for Disease Prevention and Control COVID-19. https://www.ecdc.europa.eu/en/covid-19-pandemic Available at: [accessed May 3, 2020] - PubMed
-
- Yang Y., Yang M., Shen C. Evaluating the accuracy of different respiratory specimens in the laboratory diagnosis and monitoring the viral shedding of 2019-nCoV infections. medRxiv. 2020 2020.02.11.20021493.
