

Bortezomib-based induction, high-dose melphalan and lenalidomide maintenance in myeloma up to 70 years of age
- PMID: 32684633
- PMCID: PMC8318883
- DOI: 10.1038/s41375-020-0976-9
Bortezomib-based induction, high-dose melphalan and lenalidomide maintenance in myeloma up to 70 years of age
Erratum in
-
Publisher Correction: Bortezomib-based induction, high-dose melphalan and lenalidomide maintenance in myeloma up to 70 years of age.Leukemia. 2021 Dec;35(12):3636. doi: 10.1038/s41375-021-01357-4. Leukemia. 2021. PMID: 34785794 Free PMC article. No abstract available.
Abstract
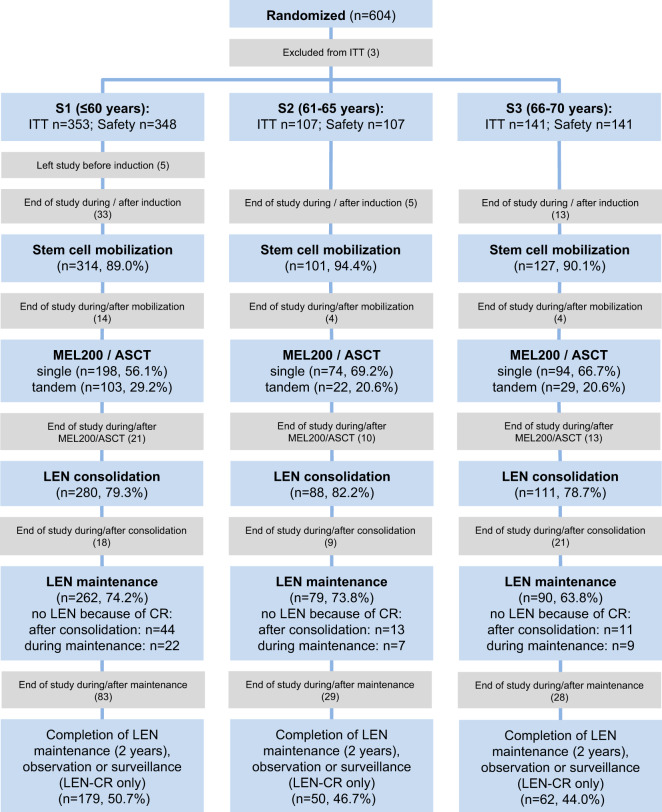
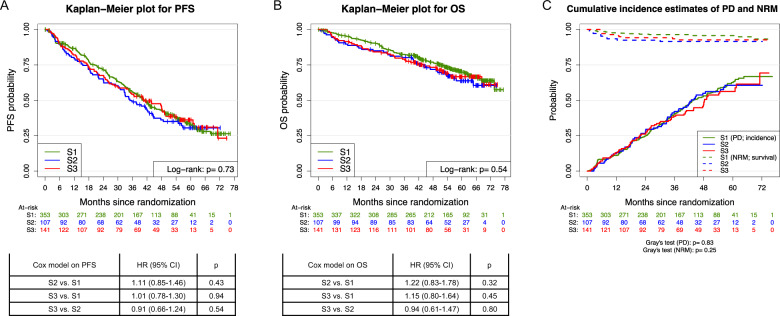
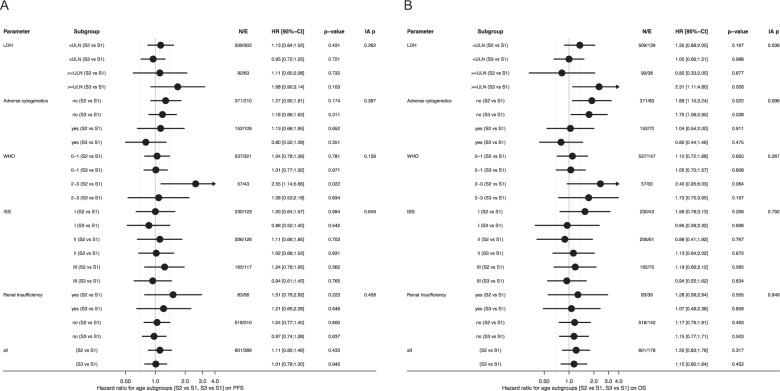
Intensive upfront therapy in newly-diagnosed multiple myeloma (MM) including induction therapy (IT), high-dose melphalan (MEL200), and autologous blood stem cell transplantation (ASCT) followed by consolidation and/or maintenance is mostly restricted to patients up to 65 years of age. Prospective phase III trial data in the era of novel agents for patients up to 70 years of age are not available. The GMMG-MM5 trial included 601 patients between 18 and 70 years of age, divided in three groups for the present analysis: ≤60 years (S1, n = 353), 61-65 years (S2, n = 107) and 66-70 years (S3, n = 141). Treatment consisted of a bortezomib-containing IT, MEL200/ASCT, consolidation, and maintenance with lenalidomide. Adherence to treatment was similar among patients of the three age groups. Overall toxicity during all treatment phases was increased in S2 and S3 compared to S1 (any adverse event/any serious adverse event: S1:81.7/41.8% vs. S2:90.7/56.5% vs. S3:87.2/68.1%, p = 0.05/<0.001). With respect to progression-free survival (log-rank p = 0.73), overall survival (log-rank p = 0.54) as well as time-to-progression (Gray's p = 0.83) and non-relapse mortality (Gray's p = 0.25), no differences were found between the three age groups. Our results imply that an intensive upfront therapy with a bortezomib-containing IT, MEL200/ASCT, lenalidomide consolidation, and maintenance should be applied to transplant-eligible MM patients up to 70 years of age.
Conflict of interest statement
EKM: honoraria: Janssen, Celgene, Takeda; consulting or advisory role: Janssen, Celgene, Takeda; research funding: Takeda; travel, accommodations, expenses: Janssen, Takeda, Celgene, Onyx, Mundipharma. KM: no COI. UB: travel, accommodations, expenses: Sanofi. JD: consulting or advisory role: Celgene; speakers bureau: Celgene; travel, accommodations, expenses: Celgene. CS: honoraria: BMS, Janssen, Celgene, Novartis, Amgen, Takeda; consulting or advisory role: BMS, Janssen, Celgene, Novartis, Amgen, Takeda; speakers bureau: Takeda; research funding: Takeda, Novartis; travel, accommodations, expenses: BMS, Janssen, Celgene, Novartis, Amgen, Takeda. KCW: honoraria: AMGEN, BMS, Celgene, Novartis, Janssen, Takeda; consulting or advisory role: AMGEN, BMS, Celgene, Juno, Janssen, Adaptive, Sanofi, Takeda; research funding: AMGEN, Celgene, Sanofi, Janssen; CK: no COI. MMu: honoraria: Janssen, BMS, Takeda, Celgene, Amgen; consulting or advisory role: Janssen, BMS, Takeda, Celgene, Amgen; research funding: BMS; travel, accommodations, expenses: Janssen, BMS, Takeda, Amgen. HWL: no COI. MMe: consulting or advisory role: Amgen, Takeda; research funding: Takeda; travel, accommodations, expenses: Celgene, AMGEN, Takeda, AbbVie, Janssen. DH: consulting or advisory role: I. Lamkap Bio AG. Discoveric AG; research funding: Celgene AG. Sanofi. Engmab AG; travel, accommodations, expenses: Celgene. AJ: no COI. AS: consulting or advisory role: I. Lamkap Bio AG. Discoveric AG; research funding: Celgene AG. Sanofi. Engmab AG. SL: no COI. SS: no COI. SF: consulting or advisory role: Sanofi, BMS, Amgen. PB: consulting or advisory role: BMS, AMGEN, Roche, MSD; research funding: BMS; travel, accommodations, expenses: BMS. AE: consulting or advisory role: Amgen; travel, accommodations, expenses: Janssen, Amgen. MG: no COI. HB: no COI. MHo: honoraria: MSD. MSR: honoraria: Celgene, BMS, Novartis, Janssen, Takeda; consulting or advisory role: Celgene, BMS, Novartis, Janssen, Takeda; research funding: Celgene, Novartis, AMGEN; travel, accommodations, expenses: Janssen, BMS, Takeda. IWB: research funding: Celgene, BMS, Janssen. MHä: honoraria: Novartis, Amgen, Roche, Takeda; consulting or advisory role: Celgene. AB: no COI. HJS: honoraria: Celgene, Janssen, Cilag; travel, accommodations, expenses: Celgene, Janssen, Cilag. HG: honoraria: Amgen, BMS, Celgene, Chugai, Janssen, Novartis, Takeda; consulting or advisory role: Amgen, BMS, Celgene, Chugai, Janssen, Novartis, Takeda; speakers bureau: Amgen, BMS, Celgene, Janssen, Novartis, Takeda; research funding: Amgen, BMS, Celgene, Chugai, Janssen, Novartis, Takeda; travel, accommodations, expenses: BMS, Celgene, Janssen, Novartis, Takeda.
Figures
References
-
- Gay F, Oliva S, Petrucci MT, Conticello C, Catalano L, Corradini P, et al. Chemotherapy plus lenalidomide versus autologous transplantation, followed by lenalidomide plus prednisone versus lenalidomide maintenance, in patients with multiple myeloma: a randomised, multicentre, phase 3 trial. Lancet Oncol. 2015;16:1617–29. - PubMed
-
- Palumbo A, Cavallo F, Gay F, Di Raimondo F, Ben Yehuda D, Petrucci MT, et al. Autologous transplantation and maintenance therapy in multiple myeloma. N Engl J Med. 2014;371:895–905. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
