

Pulmonary alveolarproteinosis in children
- PMID: 32684993
- PMCID: PMC7341618
- DOI: 10.1183/20734735.0001-2020
Pulmonary alveolarproteinosis in children
Abstract
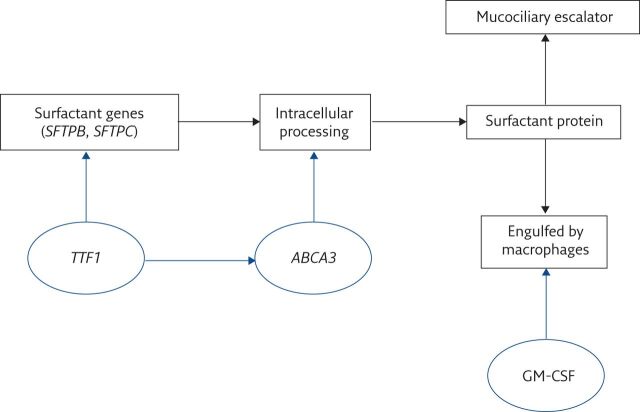
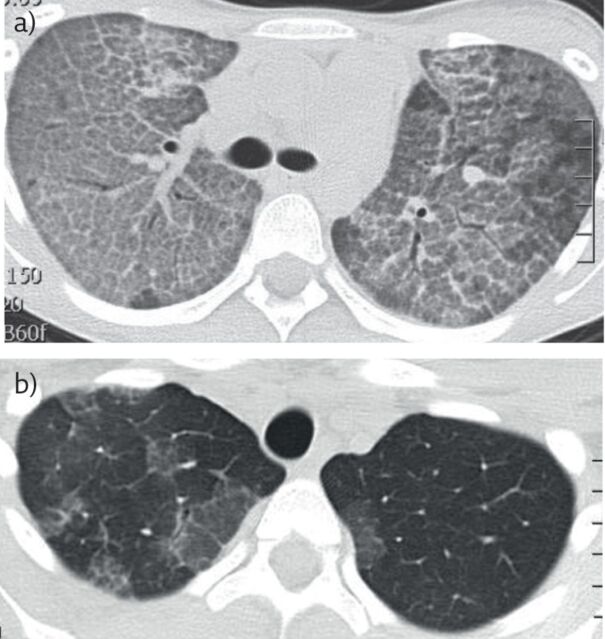
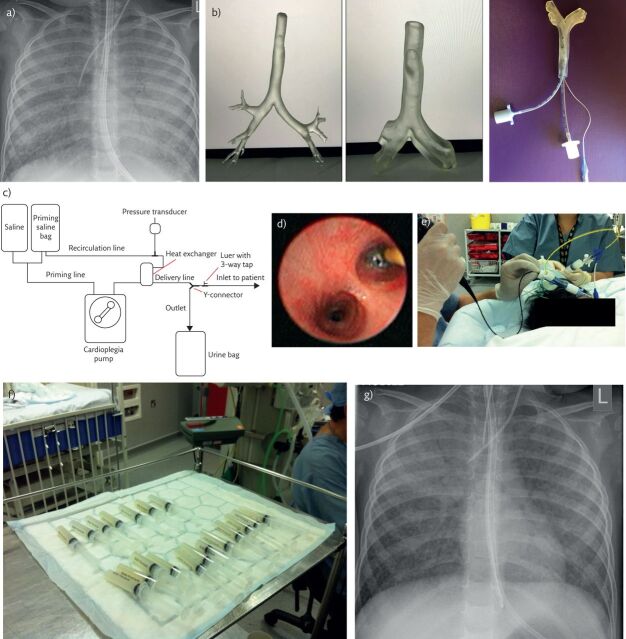
Pulmonary alveolar proteinosis (PAP) is an umbrella term for a wide spectrum of conditions that have a very characteristic appearance on computed tomography. There is outlining of the secondary pulmonary lobules on the background of ground-glass shadowing and pathologically, filling of the alveolar spaces with normal or abnormal surfactant. PAP is rare and the common causes in children are very different from those seen in adults; autoimmune PAP is rare and macrophage blockade not described in children. There are many genetic causes of PAP, the best known of which are mutations in the genes encoding surfactant protein (SP)-B, SP-C, thyroid transcription factor 1, ATP-binding cassette protein 3, and the granulocyte-macrophage colony-stimulating factor (GM-CSF) receptor α- and β- chains. PAP may also be a manifestation of rheumatological and metabolic disease, congenital immunodeficiency, and haematological malignancy. Precise diagnosis of the underlying cause is essential in planning treatment, as well as for genetic counselling. The evidence base for treatment is poor. Some forms of PAP respond well to whole-lung lavage, and autoimmune PAP, which is much commoner in adults, responds to inhaled or subcutaneous GM-CSF. Emerging therapies based on studies in murine models of PAP include stem-cell transplantation for GM-CSF receptor mutations.
Educational aims: To understand when to suspect that a child has pulmonary alveolar proteinosis (PAP) and how to confirm that this is the cause of the presentation.To show that PAP is an umbrella term for conditions characterised by alveolar filling by normal or abnormal surfactant, and that this term is the start, not the end, of the diagnostic journey.To review the developmental differences in the spectrum of conditions that may cause PAP, and specifically to understand the differences between causes in adults and children.To discuss when to treat PAP with whole-lung lavage and/or granulocyte-macrophage colony-stimulating factor, and review potential promising new therapies.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: A. Bush has nothing to disclose. Conflict of interest: R. Pabary has nothing to disclose.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials