

Inflammatory myofibroblastic tumor of the liver: A case report and review of literature
- PMID: 32685109
- PMCID: PMC7336290
- DOI: 10.4254/wjh.v12.i4.170
Inflammatory myofibroblastic tumor of the liver: A case report and review of literature
Abstract
Background: Inflammatory myofibroblastic tumors of the liver (IMTL) are extremely rare neoplasms and very little is known about their clinical presentation, pathogenesis, and biological behavior. Due to their absolute rarity, it is almost impossible to obtain a definite diagnosis without histological examination. Because of their intermediate biological behavior with the risk for local recurrence and metastases, surgical resection is recommend whenever IMTL is suspect.
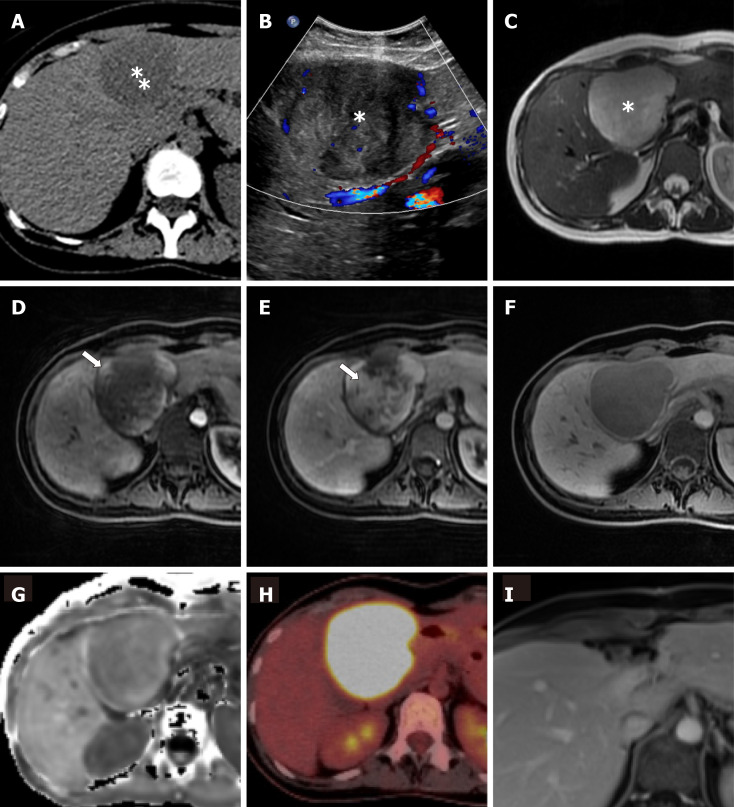
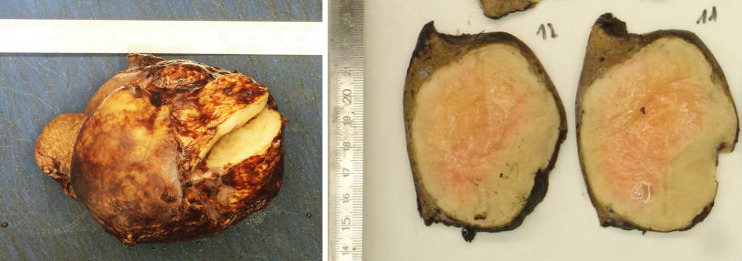
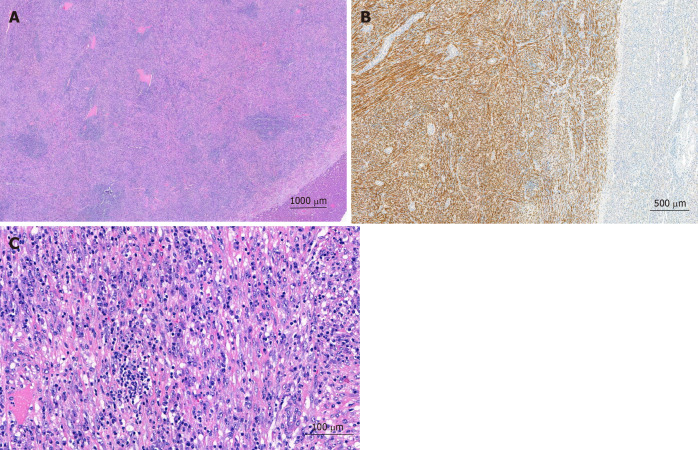
Case summary: We herein present a case of an otherwise healthy 32-year-old woman who presented with intermittent fever, unclear anemia, malaise and right flank pain 4 mo postpartum. The liver mass in segment IVa/b was highly FDG avid in the positron emission tomography-computed tomography. Hepatic resection was performed achieving a negative resection margin and an immediate resolution of all clinical symptoms. Histological analysis diagnosed the rare finding of an inflammatory myofibroblastic tumor of the liver and revealed cytoplasmic anaplastic lymphoma kinase expression by immunohistochemistry. Twelve months follow-up magnetic resonance imaging showed no recurrence and no metastases in the fully recovered patient.
Conclusion: IMTLs are extremely rare and difficult to diagnose. Due to their intermediate biological behavior, surgical resection should be perform whenever feasible and patients should be followed-up in order to detect recurrence and metastasis as early as possible.
Keywords: Anaplastic lymphoma kinase-expression; Case report; Hepatic; Inflammatory; Inflammatory myofibroblastic tumor; Review.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Figures
References
-
- Coffin CM, Watterson J, Priest JR, Dehner LP. Extrapulmonary inflammatory myofibroblastic tumor (inflammatory pseudotumor). A clinicopathologic and immunohistochemical study of 84 cases. Am J Surg Pathol. 1995;19:859–872. - PubMed
-
- Coffin CM, Humphrey PA, Dehner LP. Extrapulmonary inflammatory myofibroblastic tumor: a clinical and pathological survey. Semin Diagn Pathol. 1998;15:85–101. - PubMed
-
- Cook JR, Dehner LP, Collins MH, Ma Z, Morris SW, Coffin CM, Hill DA. Anaplastic lymphoma kinase (ALK) expression in the inflammatory myofibroblastic tumor: a comparative immunohistochemical study. Am J Surg Pathol. 2001;25:1364–1371. - PubMed
-
- Fletcher CD, Unni KK, Mertens F. Pathology and Genetics of Tumours of Soft Tissue and Bone. In: Kleihues P, Sobin LH, editors. In: Kleihues P, Sobin LH. World Health Organization Classification of Tumours. Lyon: IARC, 2002: 120-122.
-
- Jin YW, Li FY, Cheng NS. Inflammatory myofibroblastic tumor: An unusual hepatic tumor mimicking liver abscess. Clin Res Hepatol Gastroenterol. 2017;41:243–245. - PubMed
