

Homozygous LMNA p.R582H pathogenic variant reveals increasing effect on the severity of fat loss in lipodystrophy
- PMID: 32685188
- PMCID: PMC7362519
- DOI: 10.1186/s40842-020-00100-9
Homozygous LMNA p.R582H pathogenic variant reveals increasing effect on the severity of fat loss in lipodystrophy
Abstract
Background: Classical heterozygous pathogenic variants of the lamin A/C (LMNA) gene cause autosomal dominant familial partial lipodystrophy type 2 (FPLD2). However, recent reports indicate phenotypic heterogeneity among carriers of LMNA pathogenic variants, and a few patients have been associated with generalized fat loss.
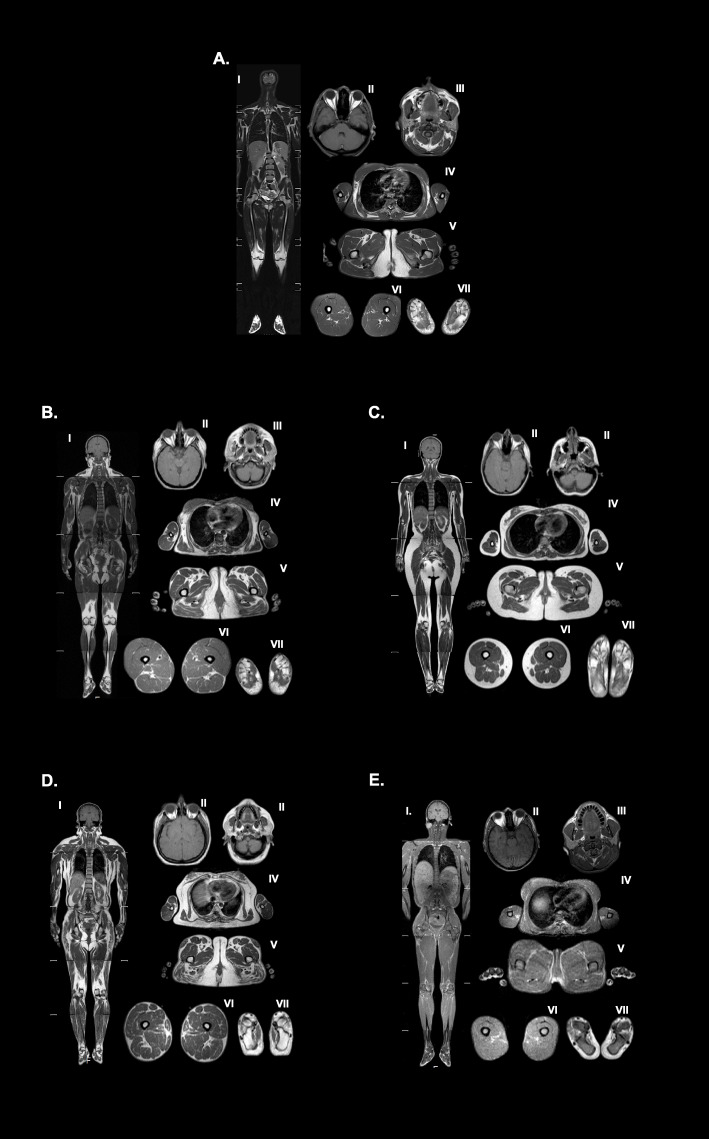
Case presentation: Here, we report a patient with a lamin A specific pathogenic variant in exon 11, denoted LMNA (c.1745G > A; p.R582H), present in the homozygous state. Fat distribution was compared radiographically to an unrelated heterozygote LMNA p.R582H patient from another pedigree, a healthy female control, a series of adult female subjects with congenital generalized lipodystrophy type 1 (CGL1, n = 9), and typical FPLD2 (n = 8). The whole-body MRI of the index case confirmed near-total loss of subcutaneous adipose tissue with well-preserved fat in the retroorbital area, palms and soles, mons pubis, and external genital region. This pattern resembled the fat loss pattern observed in CGL1 with only one difference: strikingly more fat was observed around mons pubis and the genital region. Also, the p.R582H LMNA variant in homozygous fashion was associated with lower leptin level and earlier onset of metabolic abnormalities compared to heterozygous p.R582H variant and typical FPLD2 cases. On the other hand, the heterozygous LMNA p.R582H variant was associated with partial fat loss which was similar to typical FPLD2 but less severe than the patients with the hot-spot variants at position 482.
Conclusions: Our observations and radiological comparisons demonstrate an additive effect of LMNA pathogenic variants on the severity of fat loss and add to the body of evidence that there may be complex genotype-phenotype relationships in this interesting disease known as FPLD2. Although the pathological basis for fat loss is not well understood in patients harboring pathogenic variants in the LMNA gene, our observation suggests that genetic factors modulate the extent of fat loss in LMNA associated lipodystrophy.
Keywords: Generalized lipodystrophy; Homozygous; LMNA; Lamin A; Partial lipodystrophy.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsEAO was partially supported by the Lipodystrophy Fund at University of Michigan graciously contributed by the Sopha Family and the White Point Foundation of Turkey. EAO received grant support from and served as an advisor to Amylin Pharmaceuticals LLC, Bristol-Myers Squibb, AstraZeneca and Aegerion Pharmaceuticals in the past and is currently receiving grant support directly related to Lipodystrophy Treatment from Gemphire Therapeutics, Ionis Pharmaceuticals, and Akcea Therapeutics and serving as an advisor to Akcea Therapeutics, Regeneron Pharmaceuticals. EAO is also receiving grant support from GI Dynamics in an unrelated metabolic disease area. B.A. has attended Scientific Advisory Board Meetings organized by Aegerion Pharmaceuticals and Regeneron Pharmaceuticals, and has received honoraria as a speaker from AstraZeneca, Lilly, MSD, Novartis, Novo Nordisk, Boehringer-Ingelheim, Servier, and Sanofi-Aventis. Other authors have nothing to disclose.
Figures

Similar articles
-
Deciphering the Clinical Presentations in LMNA-related Lipodystrophy: Report of 115 Cases and a Systematic Review.J Clin Endocrinol Metab. 2024 Feb 20;109(3):e1204-e1224. doi: 10.1210/clinem/dgad606. J Clin Endocrinol Metab. 2024. PMID: 37843397 Free PMC article.
-
Novel and Ultra-Rare Heterozygous Mis-sense LMNA variants causing Familial Partial Lipodystrophy.J Clin Endocrinol Metab. 2025 May 14:dgaf279. doi: 10.1210/clinem/dgaf279. Online ahead of print. J Clin Endocrinol Metab. 2025. PMID: 40367289
-
Clinical presentations, metabolic abnormalities and end-organ complications in patients with familial partial lipodystrophy.Metabolism. 2017 Jul;72:109-119. doi: 10.1016/j.metabol.2017.04.010. Epub 2017 Apr 27. Metabolism. 2017. PMID: 28641778
-
UNUSUAL PRESENTATIONS OF LMNA-ASSOCIATED LIPODYSTROPHY WITH COMPLEX PHENOTYPES AND GENERALIZED FAT LOSS: WHEN THE GENETIC DIAGNOSIS UNCOVERS NOVEL FEATURES.AACE Clin Case Rep. 2020 Mar 4;6(2):e79-e85. doi: 10.4158/ACCR-2019-0366. eCollection 2020 Mar-Apr. AACE Clin Case Rep. 2020. PMID: 32524016 Free PMC article.
-
A novel homozygous Ala529Val LMNA mutation in Turkish patients with mandibuloacral dysplasia.J Clin Endocrinol Metab. 2005 Sep;90(9):5259-64. doi: 10.1210/jc.2004-2560. Epub 2005 Jul 5. J Clin Endocrinol Metab. 2005. PMID: 15998779 Review.
Cited by
-
Deciphering the Clinical Presentations in LMNA-related Lipodystrophy: Report of 115 Cases and a Systematic Review.J Clin Endocrinol Metab. 2024 Feb 20;109(3):e1204-e1224. doi: 10.1210/clinem/dgad606. J Clin Endocrinol Metab. 2024. PMID: 37843397 Free PMC article.
-
A case of familial partial lipodystrophy type 2 masquerading as Cushing syndrome: Explaining an atypical phenotype by whole-exome sequencing.Arch Endocrinol Metab. 2025 Mar 24;69(1):e240293. doi: 10.20945/2359-4292-2024-0293. Arch Endocrinol Metab. 2025. PMID: 40130571 Free PMC article.
-
Lipodystrophic Laminopathies: From Dunnigan Disease to Progeroid Syndromes.Int J Mol Sci. 2024 Aug 28;25(17):9324. doi: 10.3390/ijms25179324. Int J Mol Sci. 2024. PMID: 39273270 Free PMC article. Review.
References
-
- Garg A, Vinaitheerthan M, Weatherall PT, Bowcock AM. Phenotypic heterogeneity in patients with familial partial lipodystrophy (dunnigan variety) related to the site of missense mutations in Lamin a/c gene. J Clin Endocrinol Metab. 2001;86(1):59–65. - PubMed
-
- Akinci B, Onay H, Demir T, Savas-Erdeve S, Gen R, Simsir IY, Keskin FE, Erturk MS, Uzum AK, Yaylali GF, et al. Clinical presentations, metabolic abnormalities and end-organ complications in patients with familial partial lipodystrophy. Metabolism. 2017;72:109–119. doi: 10.1016/j.metabol.2017.04.010. - DOI - PubMed
-
- Hussain I, Patni N, Ueda M, Sorkina E, Valerio CM, Cochran E, Brown RJ, Peeden J, Tikhonovich Y, Tiulpakov A, et al. A novel generalized Lipodystrophy-associated Progeroid syndrome due to recurrent heterozygous LMNA p.T10I mutation. J Clin Endocrinol Metab. 2018;103(3):1005–1014. doi: 10.1210/jc.2017-02078. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
