

High-Dose Inhaled Nitric Oxide as Adjunct Therapy in Cystic Fibrosis Targeting Burkholderia multivorans
- PMID: 32685229
- PMCID: PMC7334765
- DOI: 10.1155/2020/1536714
High-Dose Inhaled Nitric Oxide as Adjunct Therapy in Cystic Fibrosis Targeting Burkholderia multivorans
Abstract
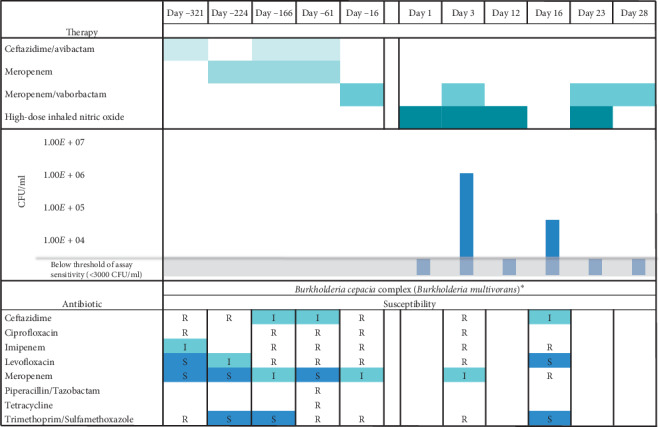
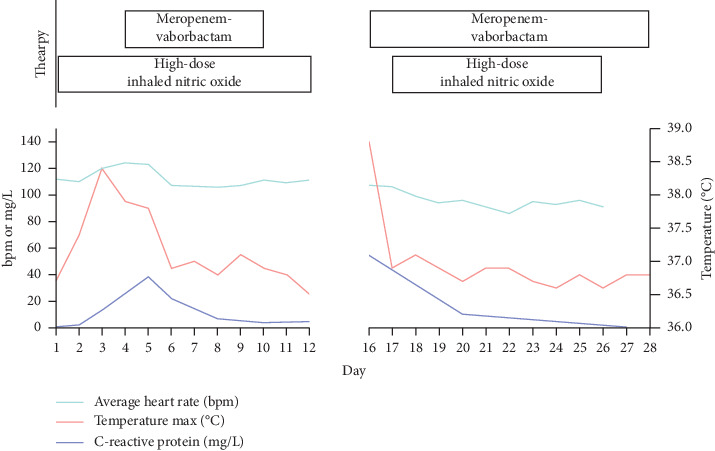
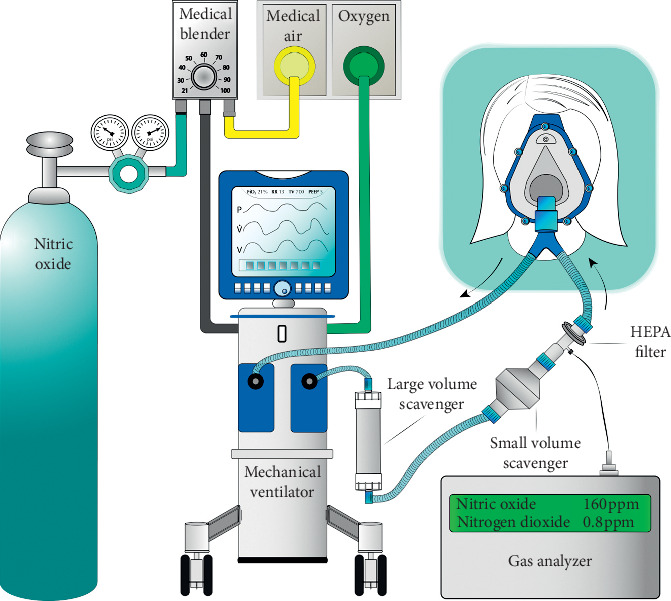
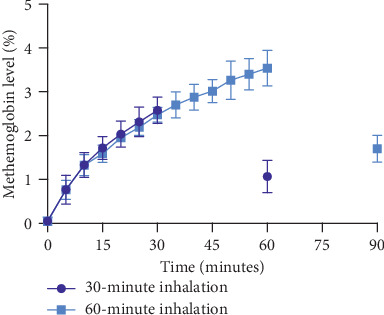
Background: Individuals with cystic fibrosis (CF) have persistent lung infections, necessitating the frequent use of antibiotics for pulmonary exacerbations. Some respiratory pathogens have intrinsic resistance to the currently available antibiotics, and any pathogen may acquire resistance over time, posing a challenge to CF care. Gaseous nitric oxide has been shown to have antimicrobial activity against a wide variety of microorganisms, including common CF pathogens, and offers a potential inhaled antimicrobial therapy. Case Presentation. Here, we present the case of a 16-year-old female with CF who experienced a precipitous decline in lung function over the prior year in conjunction with worsening antibiotic resistance of her primary pathogen, Burkholderia multivorans. She received 46 intermittent inhalations of 160 parts-per-million nitric oxide over a 28-day period. The gas was administered via a mechanical ventilator fitted with nitrogen dioxide scavenging chambers.
Conclusions: High-dose inhaled nitric oxide was safe, well tolerated, and showed clinical benefit in an adolescent with cystic fibrosis and pulmonary colonization with Burkholderia multivorans.
Copyright © 2020 Bethany L. Bartley et al.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Marshall B., Faro A., Fink A., et al. Cystic fibrosis foundation patient registry, 2017 Annual Data Report. Bethesda, MD, USA: Cystic Fibrosis Foundation; 2018. https://www.cff.org/Research/Researcher-Resources/Patient-Registry/2017-....
-
- US Food and Drug Administration. INOmax (nitric oxide) for inhalation. 2009. https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020845s009lbl.pdf.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
