

Gait Analysis after Total Knee Arthroplasty Assisted by 3D-Printed Personalized Guide
- PMID: 32685514
- PMCID: PMC7345611
- DOI: 10.1155/2020/6485178
Gait Analysis after Total Knee Arthroplasty Assisted by 3D-Printed Personalized Guide
Abstract
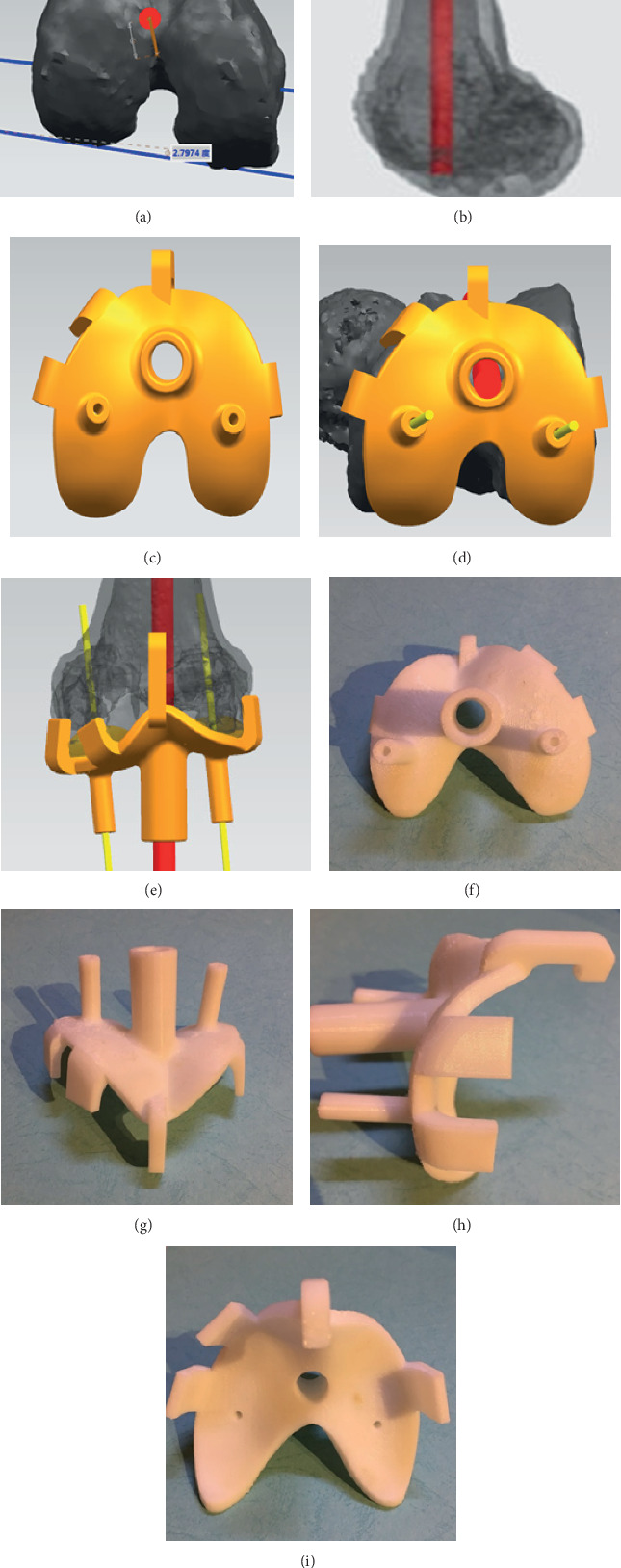
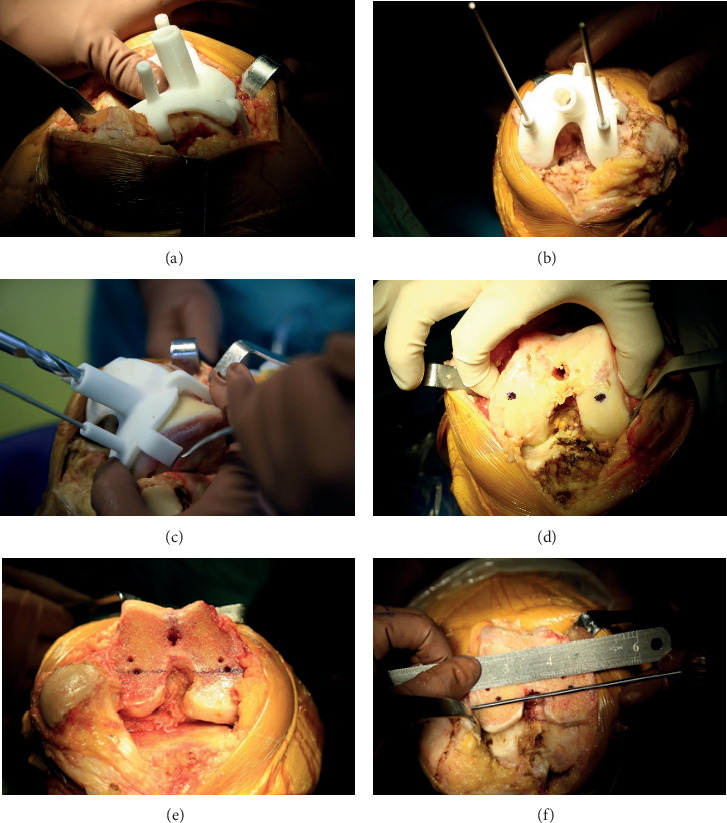
Background: With the development of three-dimensional printing (3DP) technology, the patient-specific instrumentation (PSI) has been widely applied in total knee arthroplasty (TKA). The purpose of this study was to compare the gait parameters of patients with 3DP personalized guide-assisted and standard TKA.
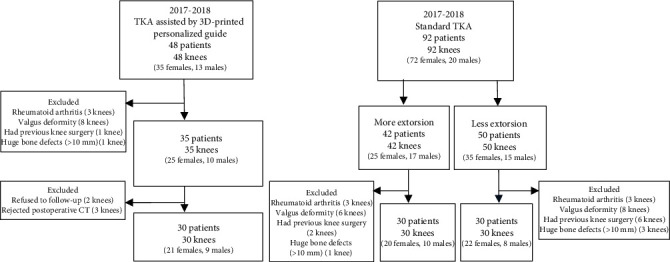
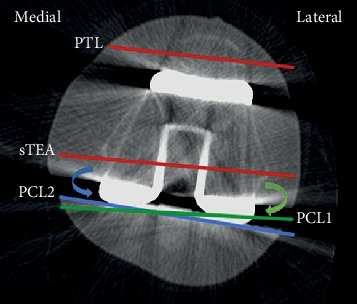
Methods: Retrospective analysis of the advanced knee OA cases in our hospital between June 2017 and June 2018 was conducted. 30 cases received 3DP personalized guide-assisted TKA (group A), and 60 patients who underwent standard TKA during the same period were in group B and group C according to the computed tomography (CT) measurement results, each with 30 cases. Hip-knee-ankle angle (HKA), patella transverse axis-femoral transepicondylar axis angle (PFA), and gait parameters were statistically analyzed. The function was assessed by Hospital for Specific Surgery (HSS) and Knee Society Score (KSS).
Results: The mean follow-up period was 12.3 months in the three groups. The knee max flexion angle at the swing phase of group A was larger than group B and group C (P < 0.05), there was no statistically significant difference in other gait parameters. The mean PFA of group A was smaller than that of group B and group C (P < 0.05). While, the HKA, HSS, and KSS scores of three groups showed no significant difference.
Conclusion: 3DP personalized guide technology could improve the gait parameters after surgery, specifically reflected in the knee max flexion angle at the swing phase. It could also assist in the reconstruction of more accurate patellar tracking and rotational alignment in TKA, avoiding the occurrence of insufficient or excessive extorsion.
Copyright © 2020 Maolin Sun et al.
Conflict of interest statement
The authors declare that there are no competing interests regarding the publication of the paper.
Figures
Similar articles
-
Accuracy of a Novel 3D-Printed Patient-Specific Intramedullary Guide to Control Femoral Component Rotation in Total Knee Arthroplasty.Orthop Surg. 2020 Apr;12(2):429-441. doi: 10.1111/os.12619. Epub 2020 Feb 22. Orthop Surg. 2020. PMID: 32087620 Free PMC article. Clinical Trial.
-
[Effect of three-dimensional printing guide plate on improving femoral rotational alignment and patellar tracking in total knee arthroplasty].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020 Mar 15;34(3):335-340. doi: 10.7507/1002-1892.201907045. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020. PMID: 32174079 Free PMC article. Clinical Trial. Chinese.
-
[Gait analysis after total knee arthroplasty assisted by three-dimensional printing navigation template].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2019 Aug 15;33(8):953-959. doi: 10.7507/1002-1892.201902068. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2019. PMID: 31407552 Free PMC article. Chinese.
-
Comparison of Kinematic Alignment and Mechanical Alignment in Total Knee Arthroplasty: A Meta-analysis of Randomized Controlled Clinical Trials.Orthop Surg. 2020 Dec;12(6):1567-1578. doi: 10.1111/os.12826. Epub 2020 Oct 25. Orthop Surg. 2020. PMID: 33099892 Free PMC article. Review.
-
Evaluation of the efficacy after Total Knee Arthroplasty by Gait analysis in patients with Knee Osteoarthritis: a meta-analysis.J Orthop Surg Res. 2024 Sep 30;19(1):612. doi: 10.1186/s13018-024-05091-2. J Orthop Surg Res. 2024. PMID: 39343975 Free PMC article.
Cited by
-
Nomogram in Knee Instability: 3D Gait Analysis of Knee Osteoarthritis Patients.Indian J Orthop. 2022 Jun 20;56(9):1554-1564. doi: 10.1007/s43465-022-00644-1. eCollection 2022 Sep. Indian J Orthop. 2022. PMID: 36052386 Free PMC article.
-
Application of three-dimensional-printed porous tantalum cones in total knee arthroplasty revision to reconstruct bone defects.Front Bioeng Biotechnol. 2022 Sep 5;10:925339. doi: 10.3389/fbioe.2022.925339. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 36131719 Free PMC article.
-
Three-Dimensional Printing of Medical Devices Used Directly to Treat Patients: A Systematic Review.3D Print Addit Manuf. 2021 Dec 1;8(6):366-408. doi: 10.1089/3dp.2020.0324. Epub 2021 Dec 9. 3D Print Addit Manuf. 2021. PMID: 36655011 Free PMC article. Review.
-
Innovations in three-dimensional-printed individualized bone prosthesis materials: revolutionizing orthopedic surgery: a review.Int J Surg. 2024 Oct 1;110(10):6748-6762. doi: 10.1097/JS9.0000000000001842. Int J Surg. 2024. PMID: 38905508 Free PMC article. Review.
-
Pressure sensing mat as an objective and sensitive tool for the evaluation of lameness in rabbits.PLoS One. 2023 Jul 7;18(7):e0286918. doi: 10.1371/journal.pone.0286918. eCollection 2023. PLoS One. 2023. PMID: 37418422 Free PMC article.
References
-
- Khlopas H., Khlopas A., Samuel L. T., et al. Current concepts in osteoarthritis of the ankle: review. Surgical Technology International. 2019;35 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
