

Epidemiology and persistence of rhinovirus in pediatric lung transplantation
- PMID: 32686323
- PMCID: PMC7900771
- DOI: 10.1111/tid.13422
Epidemiology and persistence of rhinovirus in pediatric lung transplantation
Abstract
Background: Infection with rhinovirus (HRV) occurs following pediatric lung transplantation. Prospective studies documenting frequencies, persistence, and progression of HRV in this at-risk population are lacking.
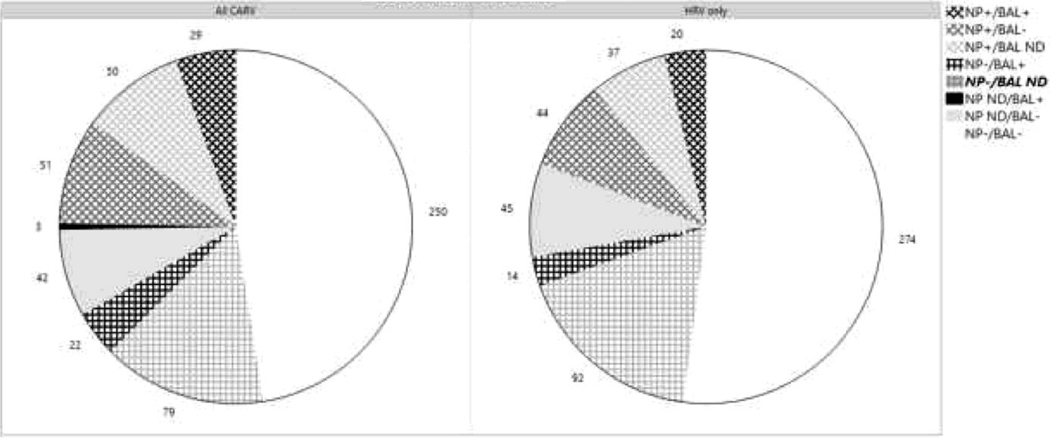
Methods: In the Clinical Trials in Organ Transplant in Children prospective observational study, we followed 61 lung transplant recipients for 2 years. We quantified molecular subtypes of HRV in serially collected nasopharyngeal (NP) and bronchoalveolar lavage (BAL) samples and correlated them with clinical characteristics.
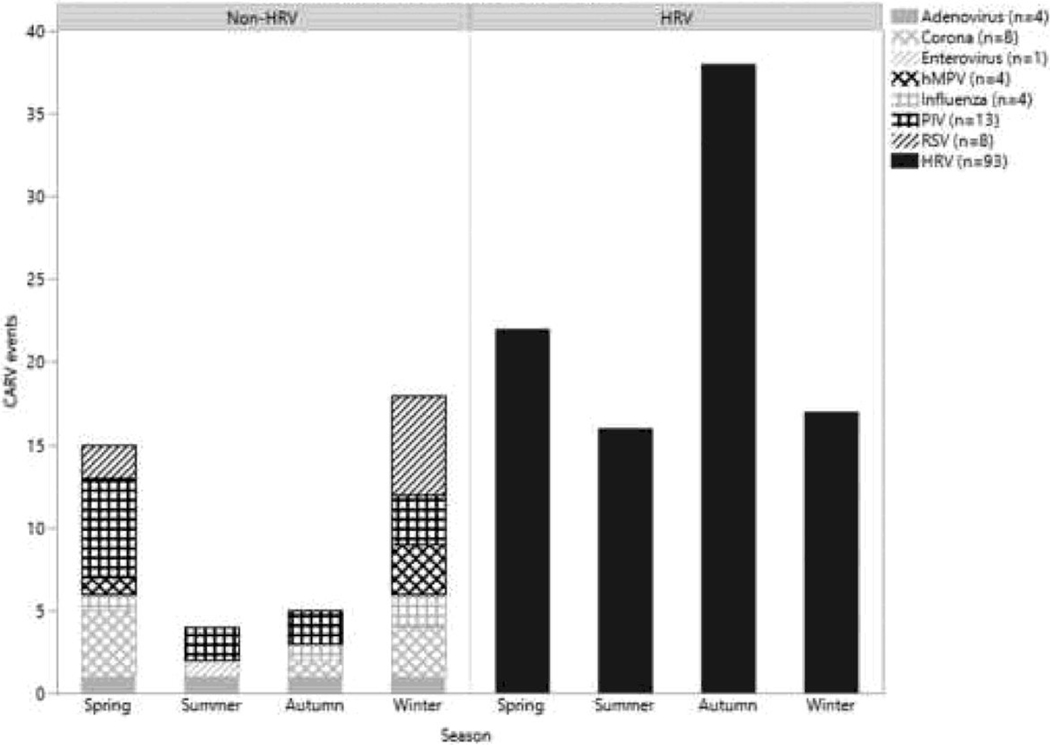
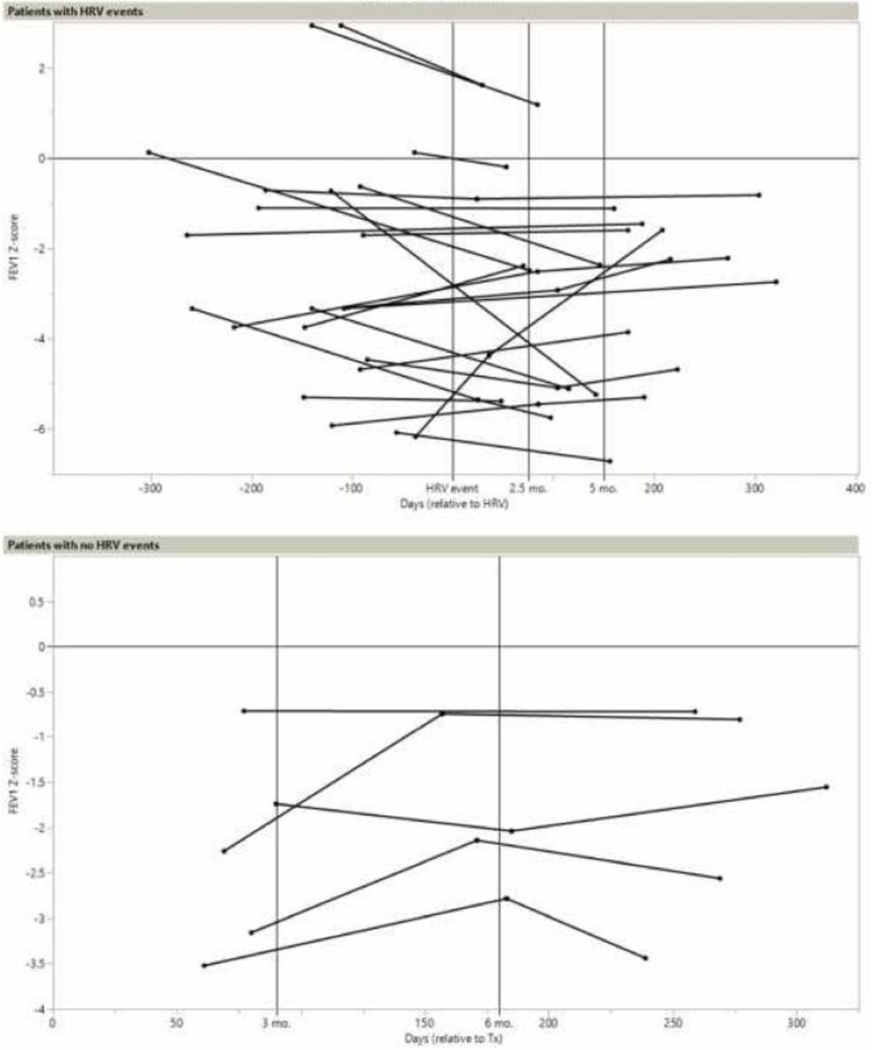
Results: We identified 135 community-acquired respiratory infections (CARV) from 397 BAL and 480 NP samples. We detected 93 HRV events in 42 (68.8%) patients, 22 of which (23.4%) were symptomatic. HRV events were contiguous with different genotypes identified in 23 cases, but symptoms were not preferentially associated with any particular species. Nine (9.7%) HRV events persisted over multiple successive samples for a median of 36 days (range 18-408 days). Three persistent HRV were symptomatic. When we serially measured forced expiratory volume in one second (FEV1) in 23 subjects with events, we did not observe significant decreases in lung function over 12 months post-HRV.
Conclusion: In conjunction with our previous reports, our prospectively collected data indicate that molecularly heterogeneous HRV infections occur commonly following pediatric lung transplantation, but these infections do not negatively impact clinical outcomes.
Keywords: community-acquired respiratory virus (CARV); forced expiratory volume (FEV1); human rhinovirus (HRV); lung transplantation; pediatrics.
© 2020 Wiley Periodicals LLC.
Conflict of interest statement
Disclosure:
The authors of this manuscript have no conflicts of interest to disclose as described by the American Journal of Transplantation.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
