

Cribriform architecture in radical prostatectomies predicts oncological outcome in Gleason score 8 prostate cancer patients
- PMID: 32686748
- PMCID: PMC7806505
- DOI: 10.1038/s41379-020-0625-x
Cribriform architecture in radical prostatectomies predicts oncological outcome in Gleason score 8 prostate cancer patients
Abstract
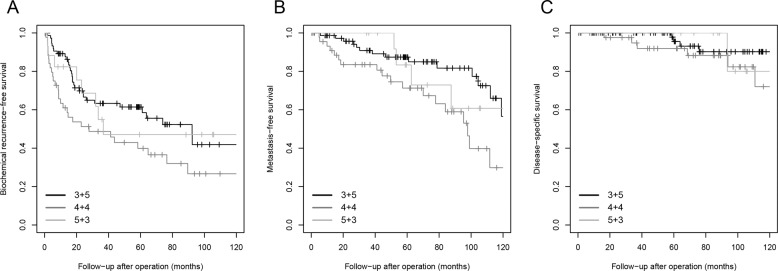
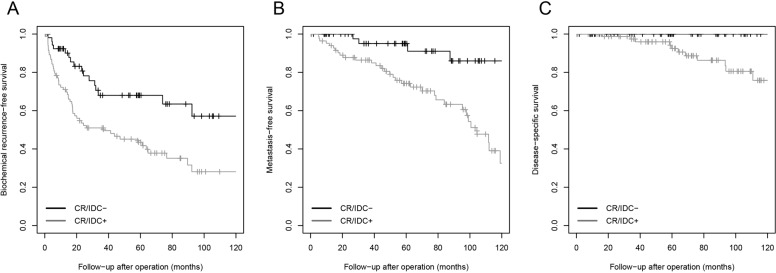
The Gleason score is an important parameter for clinical outcome in prostate cancer patients. Gleason score 8 is a heterogeneous disease including Gleason score 3 + 5, 4 + 4, and 5 + 3 tumors, and encompasses a broad range of tumor growth patterns. Our objective was to characterize individual growth patterns and identify prognostic parameters in Gleason score 8 prostate cancer patients. We reviewed 1064 radical prostatectomy specimens, recorded individual Gleason 4 and 5 growth patterns as well as presence of intraductal carcinoma, and evaluated biochemical recurrence- and metastasis-free survival. Gleason score 8 disease was identified in 140 (13%) patients, of whom 76 (54%) had Gleason score 3 + 5, 46 (33%) 4 + 4, and 18 (13%) 5 + 3 disease. Invasive cribriform and/or intraductal carcinoma (n = 87, 62%) was observed more frequently in Gleason score 4 + 4 (93%) than 3 + 5 (47%; P < 0.001) and 5 + 3 (44%; P < 0.001) patients. Gleason pattern 5 was present in 110 (79%) men: as single cells and/or cords in 99 (90%) and solid fields in 32 (29%) cases. Solid field pattern 5 coexisted with cribriform architecture (23/32, 72%) more frequently than nonsolid pattern 5 cases (36/78, 46%, P = 0.02). In multivariable analysis including age, prostate-specific antigen, pT-stage, surgical margin status, and lymph node metastases, presence of cribriform architecture was an independent parameter for biochemical recurrence-free (hazard ratio (HR) 2.0, 95% confidence interval (CI) 1.0-3.7; P = 0.04) and metastasis-free (HR 3.5, 95% CI 1.0-12.3; P = 0.05) survival. In conclusion, invasive cribriform and/or intraductal carcinoma occurs more frequently in Gleason score 4 + 4 prostate cancer patients than in Gleason score 3 + 5 and 5 + 3, and is an independent parameter for biochemical recurrence and metastasis. Therefore, cribriform architecture has added value in risk stratification of Gleason score 8 prostate cancer patients.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Gleason DF. Classification of prostatic carcinomas. Cancer Chemother Rep. 1966;50:125–8. - PubMed
-
- Epstein JI, Egevad L, Amin MB, Delahunt B, Srigley JR, Humphrey PA, et al. The 2014 International Society of Urological Pathology (ISUP) consensus conference on gleason grading of prostatic carcinoma: definition of grading patterns and proposal for a new grading system. Am J Surg Pathol. 2016;40:244–52. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
