A Pooled Analysis of Diffusion-Weighted Imaging Lesions in Patients With Acute Intracerebral Hemorrhage
- PMID: 32687564
- PMCID: PMC7372494
- DOI: 10.1001/jamaneurol.2020.2349
A Pooled Analysis of Diffusion-Weighted Imaging Lesions in Patients With Acute Intracerebral Hemorrhage
Abstract
Importance: The etiology and significance of diffusion-weighted imaging (DWI) lesions in patients with acute intracerebral hemorrhage (ICH) remain unclear.
Objective: To evaluate which factors are associated with DWI lesions, whether associated factors differ by ICH location, and whether DWI lesions are associated with functional outcomes.
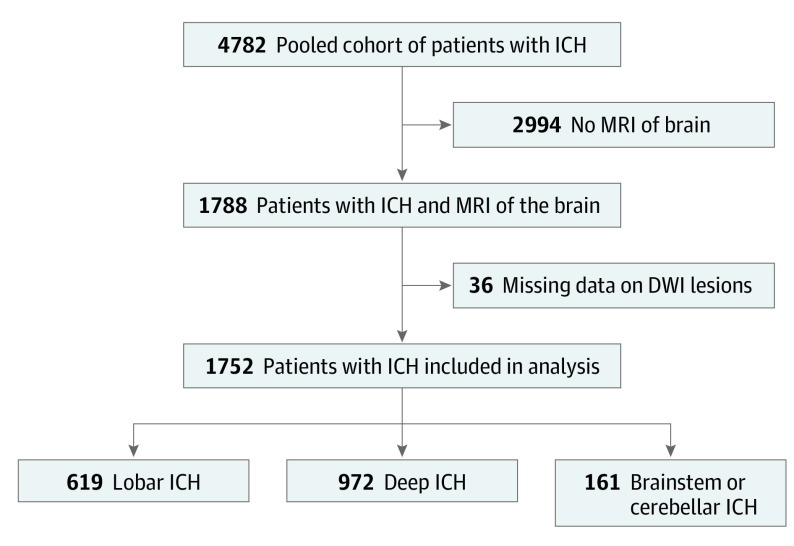
Design, setting, and participants: This analysis pooled individual patient data from 3 randomized clinical trials (Minimally Invasive Surgery Plus Alteplase for Intracerebral Hemorrhage Evacuation phase 3 trial, Antihypertensive Treatment of Acute Cerebral Hemorrhage trial, and Intracerebral Hemorrhage Deferoxamine phase 2 trial) and 1 multicenter prospective study (Ethnic/Racial Variations of Intracerebral Hemorrhage). Patients were enrolled from August 1, 2010, to September 30, 2018. Of the 4782 patients, 1788 who underwent magnetic resonance imaging scans of the brain were included. Data were analyzed from July 1 to December 31, 2019.
Main outcomes and measures: The primary outcome consisted of factors associated with DWI lesions. Secondary outcomes were poor functional outcome, defined as a modified Rankin score (mRS) of 4 to 6, and mortality, both assessed at 3 months. Mixed-effects logistic regression was used to evaluate the association between exposures and outcomes. Subgroup analyses stratified by hematoma location were performed.
Results: After exclusion of 36 patients with missing data on DWI lesions, 1752 patients were included in the analysis (1019 men [58.2%]; mean [SD] age, 60.8 [13.3] years). Diffusion-weighted imaging lesions occurred in 549 patients (31.3%). In mixed-effects regression models, factors associated with DWI lesions included younger age (odds ratio [OR] per year, 0.98; 95% CI, 0.97-0.99), black race (OR, 1.64; 95% CI, 1.17-2.30), admission systolic blood pressure (OR per 10-mm Hg increase, 1.13; 95% CI, 1.08-1.18), baseline hematoma volume (OR per 10-mL increase, 1.12; 95% CI, 1.02-1.22), cerebral microbleeds (OR, 1.85; 95% CI, 1.39-2.46), and leukoaraiosis (OR, 1.59; 95% CI, 1.67-2.17). Diffusion-weighted imaging lesions were independently associated with poor mRS (OR, 1.50; 95% CI, 1.13-2.00), but not with mortality (OR, 1.11; 95% CI, 0.72-1.71). In subgroup analyses, similar factors were associated with DWI lesions in lobar and deep ICH. Diffusion-weighted imaging lesions were associated with poor mRS in deep but not lobar ICH.
Conclusions and relevance: In a large, heterogeneous cohort of prospectively identified patients with ICH, results were consistent with the hypothesis that DWI lesions represent acute sequelae of chronic cerebral small vessel disease, particularly hypertensive vasculopathy. Diffusion-weighted imaging lesions portend a worse prognosis after ICH, mainly deep hemorrhages.
Conflict of interest statement
Figures