

Three-year outcome after transanal versus laparoscopic total mesorectal excision in locally advanced rectal cancer: a multicenter comparative analysis
- PMID: 32689968
- PMCID: PMC7372845
- DOI: 10.1186/s12885-020-07171-y
Three-year outcome after transanal versus laparoscopic total mesorectal excision in locally advanced rectal cancer: a multicenter comparative analysis
Abstract
Background: For patients with mid and distal rectal cancer, robust evidence on long-term outcome and causal treatment effects of transanal total mesorectal excision (TaTME) is lacking. This multicentre retrospective cohort study aimed to assess whether TaTME reduces locoregional recurrence rate compared to laparoscopic total mesorectal excision (LapTME).
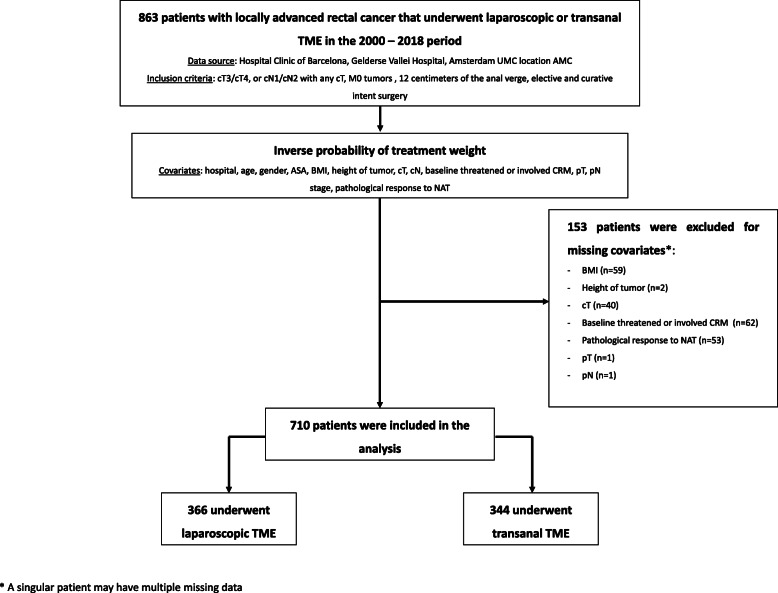
Methods: Consecutive patients with rectal cancer within 12 cm from the anal verge and clinical stage II-III were selected from three institutional databases. Outcome after TaTME (Nov 2011 - Feb 2018) was compared to a historical cohort of patients treated with LapTME (Jan 2000 - Feb 2018) using the inverse probability of treatment weights method. The primary endpoint was three-year locoregional recurrence.
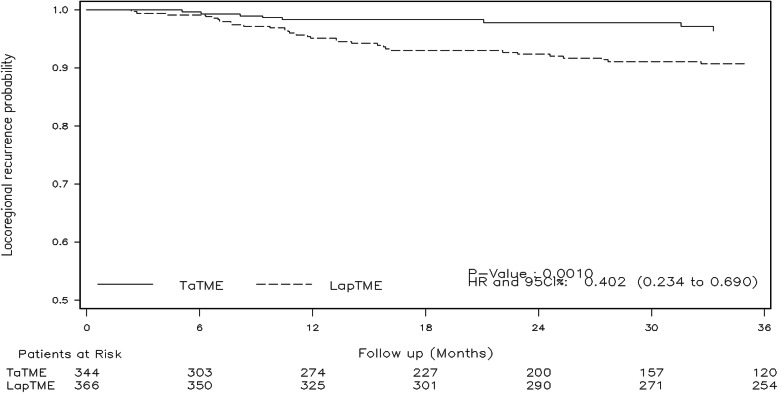
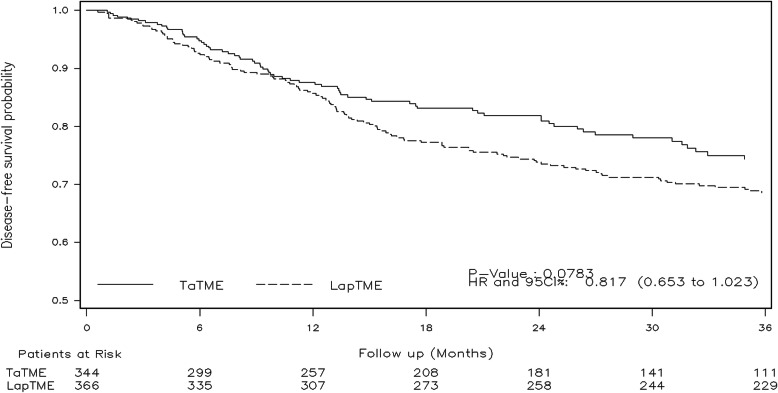
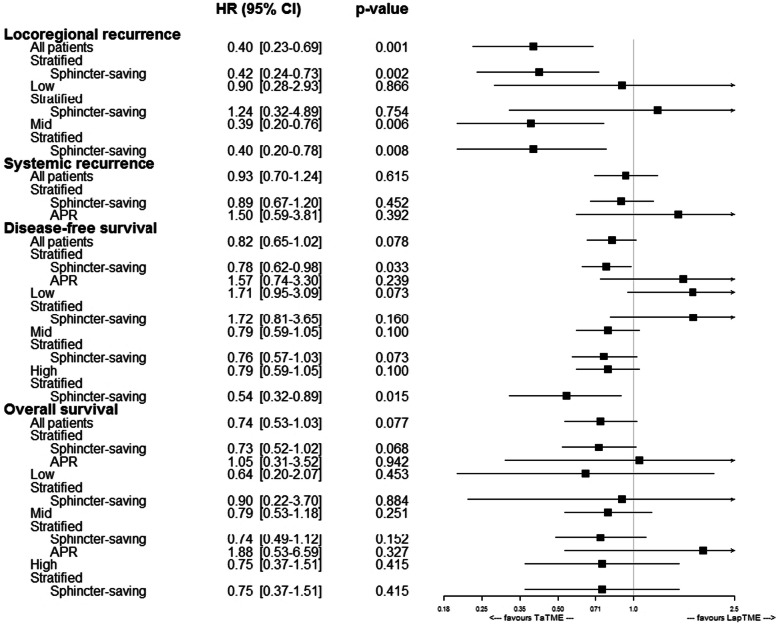
Results: A total of 710 patients were analysed, 344 in the TaTME group and 366 in the LapTME group. At 3 years, cumulative locoregional recurrence rates were 3.6% (95% CI, 1.1-6.1) in the TaTME group and 9.6% (95% CI, 6.5-12.7) in the LapTME group (HR = 0.4; 95% CI, 0.23-0.69; p = 0.001). Three-year cumulative disease-free survival rates were 74.3% (95% CI, 68.8-79.8) and 68.6% (95% CI, 63.7-73.5) (HR = 0.82; 95% CI, 0.65-1.02; p = 0.078) and three-year overall survival 87.2% (95% CI, 82.7-91.7) and 82.2% (95% CI, 78.0-86.2) (HR = 0.74; 95% CI, 0.53-1.03; p = 0.077), respectively. In patients who underwent sphincter preservation procedures, TaTME was associated with a significantly better disease-free survival (HR = 0.78; 95% CI, 0.62-0.98; p = 0.033).
Conclusions: These findings suggest that TaTME may improve locoregional recurrence and disease-free survival rates among patients with mid and distal locally advanced rectal cancer.
Keywords: Locoregional recurrence; Rectal cancer; TaTME; Total mesorectal excision.
Conflict of interest statement
Dr. F. Borja de Lacy, Drs. Sapho Xenia Roodbeen, Mr. Jose Ríos, Dr. Jacqueline van Laarhoven, Dr. Ana Otero-Piñeiro, Dr. Raquel Bravo, Dr. Tjaakje Visser, Dr. Roy van Poppel, and Dr. Silvia Valverde have no conflicts of interest or financial ties to disclose. Dr. Roel Hompes reports an educational grant from Stryker, personal fees from Applied Medical outside the submitted work. Dr. Colin Sietses reports personal fees from Medtronic, personal fees from Olympus, and personal fees from AFS medical, outside the submitted work. Dr. Antoni Castells reports personal fees from Amadix, Goodgut and Universal Diagnostics, and grants from SAF2014 and AECC, outside the submitted work. Dr. Willem A. Bemelman reports grants from VIFOR, grants from Medtronic, and grants from Braun, outside the submitted work. Dr. Pieter J. Tanis reports personal fees from Johnson & Johnson, personal fees from Olympus, and personal fees from B Braun, and research grant from Life Cell, outside the submitted work. Dr. Antonio M. Lacy reports personal fees from Medtronic, personal fees from Olympus, personal fees from Applied Medical, and personal fees from Conmed, outside the submitted work.
Figures
Similar articles
-
Outcomes of open vs laparoscopic vs robotic vs transanal total mesorectal excision (TME) for rectal cancer: a network meta-analysis.Tech Coloproctol. 2023 May;27(5):345-360. doi: 10.1007/s10151-022-02739-1. Epub 2022 Dec 12. Tech Coloproctol. 2023. PMID: 36508067 Review.
-
Transanal (TaTME) vs. laparoscopic total mesorectal excision for mid and low rectal cancer: a propensity score-matched analysis of early and long-term outcomes.Int J Colorectal Dis. 2021 Oct;36(10):2271-2279. doi: 10.1007/s00384-021-04019-0. Epub 2021 Sep 1. Int J Colorectal Dis. 2021. PMID: 34467413
-
[Safety and prognosis analysis of transanal total mesorectal excision versus laparoscopic mesorectal excision for mid-low rectal cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2022 Jun 25;25(6):522-530. doi: 10.3760/cma.j.cn441530-20210811-00321. Zhonghua Wei Chang Wai Ke Za Zhi. 2022. PMID: 35754217 Chinese.
-
Residual mesorectum on postoperative magnetic resonance imaging following transanal total mesorectal excision (TaTME) and laparoscopic total mesorectal excision (LapTME) in rectal cancer.Surg Endosc. 2019 Jan;33(1):94-102. doi: 10.1007/s00464-018-6279-9. Epub 2018 Jul 2. Surg Endosc. 2019. PMID: 29967990 Free PMC article.
-
Comparison of short-term clinical outcomes between transanal and laparoscopic total mesorectal excision for the treatment of mid and low rectal cancer: A meta-analysis.Eur J Surg Oncol. 2016 Dec;42(12):1841-1850. doi: 10.1016/j.ejso.2016.09.002. Epub 2016 Sep 19. Eur J Surg Oncol. 2016. PMID: 27697315 Review.
Cited by
-
What Is the Comparative Efficacy of Surgical, Endoscopic, Transanal Resection, and Radiotherapy Modalities in the Treatment of Rectal Cancer?Healthcare (Basel). 2023 Aug 20;11(16):2347. doi: 10.3390/healthcare11162347. Healthcare (Basel). 2023. PMID: 37628544 Free PMC article. Review.
-
Efficacy of transperineal minimally invasive surgery with laparoscopic abdominoperineal excision for lower rectal cancer.Surg Today. 2023 Apr;53(4):490-498. doi: 10.1007/s00595-022-02597-2. Epub 2022 Oct 18. Surg Today. 2023. PMID: 36255499
-
UEG and EAES rapid guideline: Systematic review, meta-analysis, GRADE assessment and evidence-informed European recommendations on TaTME for rectal cancer.Surg Endosc. 2022 Apr;36(4):2221-2232. doi: 10.1007/s00464-022-09090-4. Epub 2022 Feb 25. Surg Endosc. 2022. PMID: 35212821 Free PMC article.
-
Transanal total mesorectal excision: short- and long-term results of four certified colorectal cancer centers in Germany.Int J Colorectal Dis. 2024 Aug 15;39(1):132. doi: 10.1007/s00384-024-04704-w. Int J Colorectal Dis. 2024. PMID: 39145821 Free PMC article.
-
Oncologic outcomes following transanal total mesorectal excision: the United States experience.Surg Endosc. 2024 Jul;38(7):3703-3715. doi: 10.1007/s00464-024-10896-7. Epub 2024 May 23. Surg Endosc. 2024. PMID: 38782828
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
