

Adaptive interventions for optimizing malaria control: an implementation study protocol for a block-cluster randomized, sequential multiple assignment trial
- PMID: 32690063
- PMCID: PMC7372887
- DOI: 10.1186/s13063-020-04573-y
Adaptive interventions for optimizing malaria control: an implementation study protocol for a block-cluster randomized, sequential multiple assignment trial
Abstract
Background: In the past two decades, the massive scale-up of long-lasting insecticidal nets (LLINs) and indoor residual spraying (IRS) has led to significant reductions in malaria mortality and morbidity. Nonetheless, the malaria burden remains high, and a dozen countries in Africa show a trend of increasing malaria incidence over the past several years. This underscores the need to improve the effectiveness of interventions by optimizing first-line intervention tools and integrating newly approved products into control programs. Because transmission settings and vector ecologies vary from place to place, malaria interventions should be adapted and readapted over time in response to evolving malaria risks. An adaptive approach based on local malaria epidemiology and vector ecology may lead to significant reductions in malaria incidence and transmission risk.
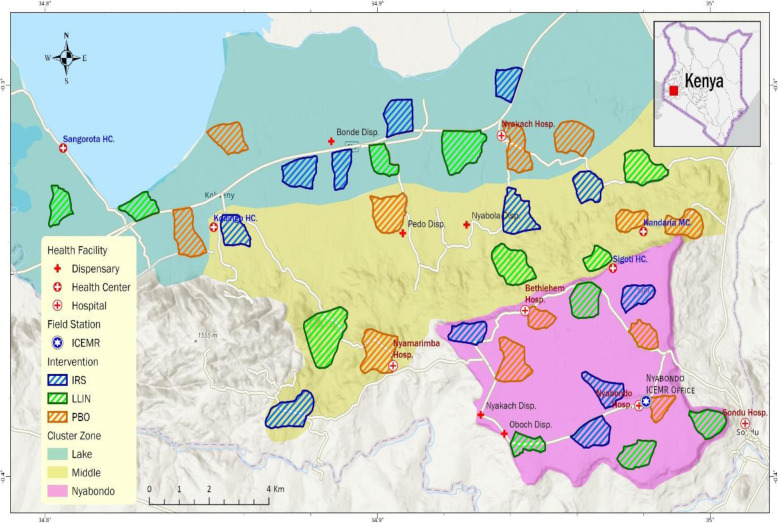
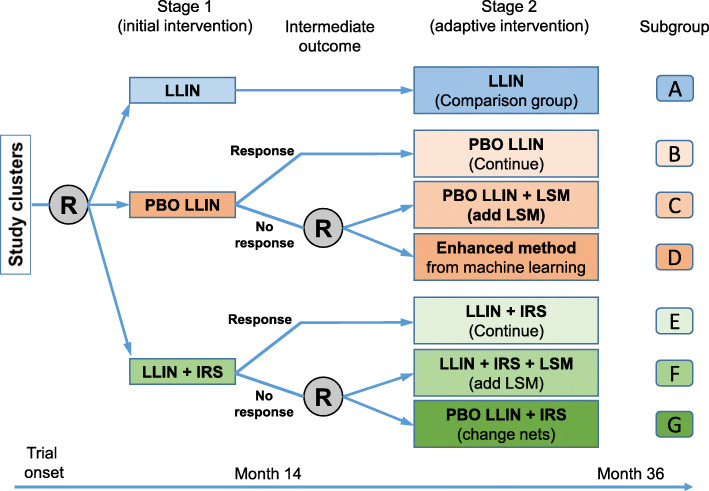
Methods/design: This study will use a longitudinal block-cluster sequential multiple assignment randomized trial (SMART) design with longitudinal outcome measures for a period of 3 years to develop an adaptive intervention for malaria control in western Kenya, the first adaptive trial for malaria control. The primary outcome is clinical malaria incidence rate. This will be a two-stage trial with 36 clusters for the initial trial. At the beginning of stage 1, all clusters will be randomized with equal probability to either LLIN, piperonyl butoxide-treated LLIN (PBO Nets), or LLIN + IRS by block randomization based on their respective malaria risks. Intervention effectiveness will be evaluated with 12 months of follow-up monitoring. At the end of the 12-month follow-up, clusters will be assessed for "response" versus "non-response" to PBO Nets or LLIN + IRS based on the change in clinical malaria incidence rate and a pre-defined threshold value of cost-effectiveness set by the Ministry of Health. At the beginning of stage 2, if an intervention was effective in stage 1, then the intervention will be continued. Non-responders to stage 1 PBO Net treatment will be randomized equally to either PBO Nets + LSM (larval source management) or an intervention determined by an enhanced reinforcement learning method. Similarly, non-responders to stage 1 LLIN + IRS treatment will be randomized equally to either LLIN + IRS + LSM or PBO Nets + IRS. There will be an 18-month evaluation follow-up period for stage 2 interventions. We will monitor indoor and outdoor vector abundance using light traps. Clinical malaria will be monitored through active case surveillance. Cost-effectiveness of the interventions will be assessed using Q-learning.
Discussion: This novel adaptive intervention strategy will optimize existing malaria vector control tools while allowing for the integration of new control products and approaches in the future to find the most cost-effective malaria control strategies in different settings. Given the urgent global need for optimization of malaria control tools, this study can have far-reaching implications for malaria control and elimination.
Trial registration: US National Institutes of Health, study ID NCT04182126 . Registered on 26 November 2019.
Keywords: Active case surveillance; Adaptive intervention; Block-cluster randomized; Clinical malaria incidence rate; Cost-effectiveness; Indoor residual spraying; Larval source management; Long-lasting insecticidal net (LLIN); Piperonyl butoxide-treated LLIN; Q-learning; Sequential multiple assignment randomized trial.
Conflict of interest statement
Ethical clearance has been obtained from the Ethical Review Committee of Maseno University, Kenya (MSU/DRPI/MUERC/00778/19), and the Institutional Review Board (IRB) of the University of California, Irvine, USA (HS# 2017-3512). Written consent will be obtained from all study participants. Written assent for children (< 18 years of age) will be obtained from the participants and their parents or guardians. Inclusion criteria are as follows: provision of informed consent (assent for children) and no reported chronic or acute illness other than malaria. Exclusion criteria are as follows: unwillingness to participate in the study or reported chronic or acute illness other than malaria. Permission to use microbial larvicides for malaria vector control has been obtained from the Pest Control Products Board of Kenya. All investigative team members in the USA and Kenya have no financial conflict of interest with the larvicide manufacturer, Central Life Sciences.
The authors declare that they have no competing interests.
Figures
References
-
- WHO . World Malaria Report 2018. Geneva: World Health Organization; 2019.
-
- Ministry of Public Health of Kenya. The Kenya Malaria Strategy 2009–2018 (Revised 2014). Ministry of Health, Kenya; 2014. http://globalfundkcm.or.ke/wp-content/uploads/2016/06/Revised-Kenya-Stra.... Accessed 30 Jan 2020.
-
- Abate A, Hadis M. Susceptibility of Anopheles gambiae s.l. to DDT, malathion, permethrin and deltamethrin in Ethiopia. Trop Med Int Health. 2011;16:486–491. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
