

Randomised phase II trial of CAPTEM or FOLFIRI as SEcond-line therapy in NEuroendocrine CArcinomas and exploratory analysis of predictive role of PET/CT imaging and biological markers (SENECA trial): a study protocol
- PMID: 32690499
- PMCID: PMC7371236
- DOI: 10.1136/bmjopen-2019-034393
Randomised phase II trial of CAPTEM or FOLFIRI as SEcond-line therapy in NEuroendocrine CArcinomas and exploratory analysis of predictive role of PET/CT imaging and biological markers (SENECA trial): a study protocol
Abstract
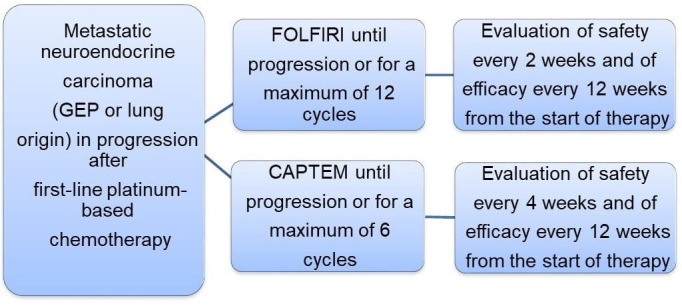
Introduction: Patients with metastatic or locally advanced, non-resectable, grade 3 poorly differentiated gastroenteropancreatic (GEP) and lung neuroendocrine carcinomas (NECs) are usually treated with in first-line platinum compounds. There is no standard second-line treatment on progression. Accurate biomarkers are needed to facilitate diagnosis and prognostic assessment of patients with NEC.
Methods and analysis: The SEcond-line therapy in NEuroendocrine CArcinomas (SENECA) study is a randomised, non-comparative, multicentre phase II trial designed to evaluate the efficacy and safety of folinic acid, 5-fluorouracil and irinotecan (FOLFIRI) or capecitabine plus temozolomide (CAPTEM) regimens after failure of first-line chemotherapy in patients with lung NEC and GEP-NEC. Secondary aims are to correlate the serum miRNA profile and primary mutational status of MEN1, DAXX, ATRX and RB-1 with prognosis and outcome and to investigate the prognostic and predictive role of the Ki-67 score and 18-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) or 68Ga-PET/CT. The main eligibility criteria are age ≥18 years; metastatic or locally advanced, non-resectable, grade 3 lung or GEP-NECs; progression to first-line platinum-based chemotherapy. A Bryant and Day design taking into account treatment activity and toxicity was used to estimate the sample size. All analyses will be performed separately for each treatment group in the intention-to-treat population. A total of 112 patients (56/arm) will be randomly assigned (1:1) to receive FOLFIRI every 14 days or CAPTEM every 28 days until disease progression or unacceptable toxicity or for a maximum of 6 months. Patients undergo testing for specific biomarkers in primary tumour tissue and for miRNA in blood samples. MiRNA profiling will be performed in the first 20 patients who agree to participate in the biological substudy.
Ethics and dissemination: The SENECA trial, supported by Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori (IRST), was authorised by the locals Ethics Committee and the Italian Medicines Agency (AIFA). Results will be widely disseminated via peer-reviewed manuscripts, conference presentations and reports to relevant authorities.The study is currently open in Italy.
Trail registration number: NCT03387592; Pre-results. EudraCT-2016-000767-17.
Protocol version: Clinical Study Protocol Version 1, 7 November 2016.
Keywords: CAPTEM; FOLFIRI; capecitabine, temozolomide; neuroendocrine carcinoma; second-line.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Lloyd RV, Osamura RY, Klöppel G, et al. . WHO classification of tumours of endocrine organs. 4th edn Lyon: International Agency for Research on Cancer (IARC), 2017.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous