

Immune Surveillance in Clinical Regression of Preinvasive Squamous Cell Lung Cancer
- PMID: 32690541
- PMCID: PMC7611527
- DOI: 10.1158/2159-8290.CD-19-1366
Immune Surveillance in Clinical Regression of Preinvasive Squamous Cell Lung Cancer
Abstract
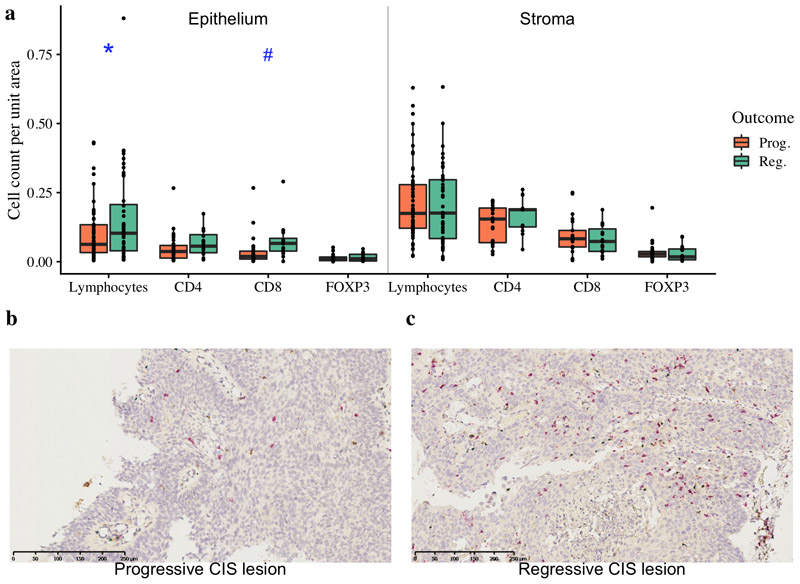
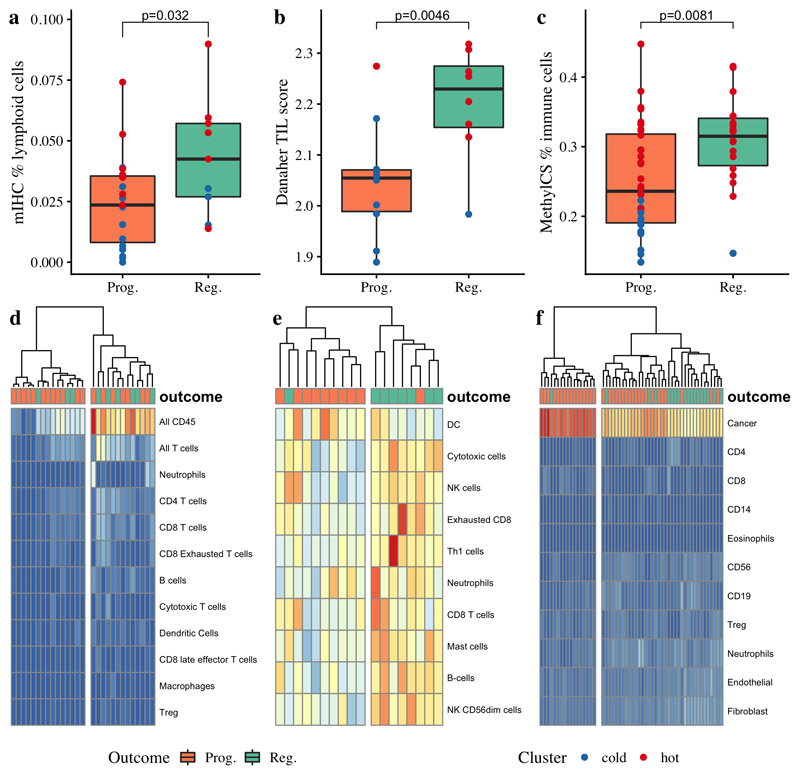
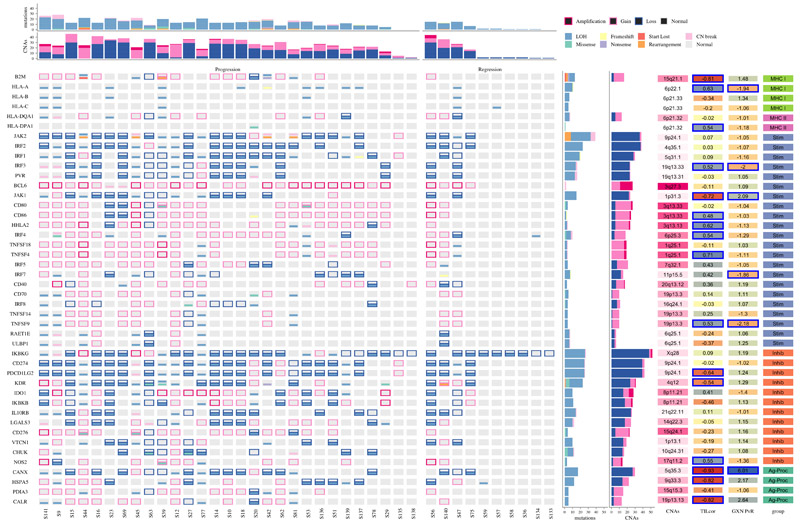
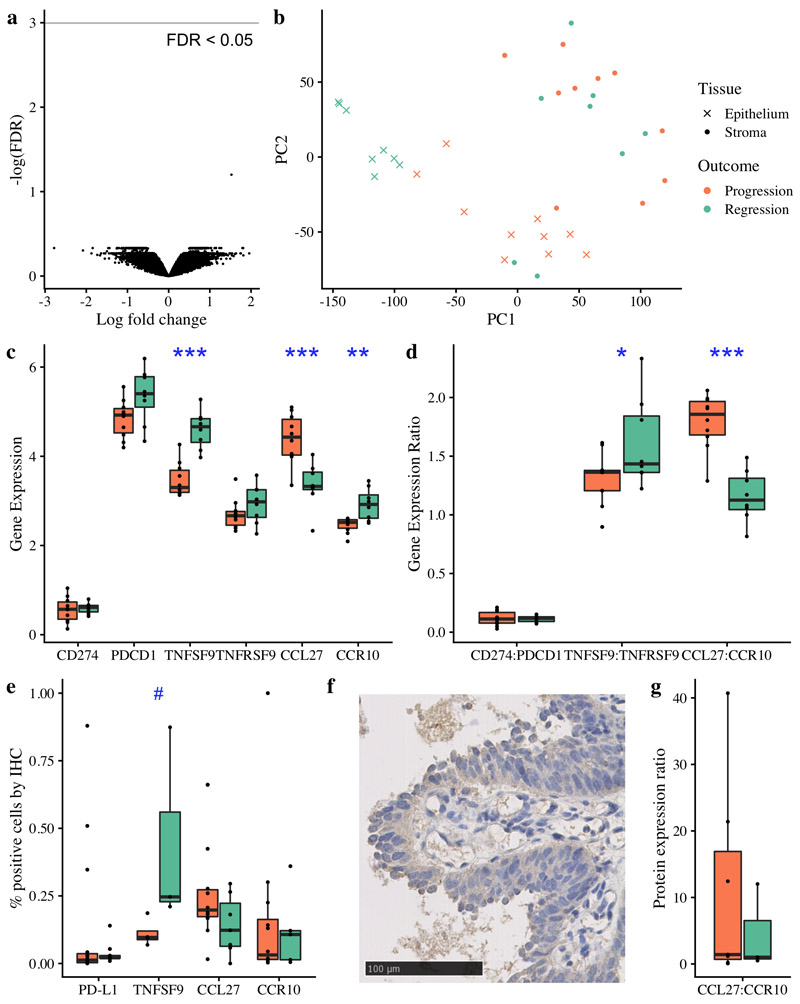
Before squamous cell lung cancer develops, precancerous lesions can be found in the airways. From longitudinal monitoring, we know that only half of such lesions become cancer, whereas a third spontaneously regress. Although recent studies have described the presence of an active immune response in high-grade lesions, the mechanisms underpinning clinical regression of precancerous lesions remain unknown. Here, we show that host immune surveillance is strongly implicated in lesion regression. Using bronchoscopic biopsies from human subjects, we find that regressive carcinoma in situ lesions harbor more infiltrating immune cells than those that progress to cancer. Moreover, molecular profiling of these lesions identifies potential immune escape mechanisms specifically in those that progress to cancer: antigen presentation is impaired by genomic and epigenetic changes, CCL27-CCR10 signaling is upregulated, and the immunomodulator TNFSF9 is downregulated. Changes appear intrinsic to the carcinoma in situ lesions, as the adjacent stroma of progressive and regressive lesions are transcriptomically similar. SIGNIFICANCE: Immune evasion is a hallmark of cancer. For the first time, this study identifies mechanisms by which precancerous lesions evade immune detection during the earliest stages of carcinogenesis and forms a basis for new therapeutic strategies that treat or prevent early-stage lung cancer.See related commentary by Krysan et al., p. 1442.This article is highlighted in the In This Issue feature, p. 1426.
©2020 American Association for Cancer Research.
Conflict of interest statement
S.A.Q. and C.S. are co-founders of Achilles Therapeutics. C.S. is a shareholder of Apogen Biotechnologies, Epic Bioscience, GRAIL, and has stock options in Achilles Therapeutics. R.R. and N.M. have stock options in and have consulted for Achilles Therapeutics. L.M.C. is a paid consultant for Cell Signaling Technologies, received reagent and/or research support from Plexxikon Inc., Pharmacyclics, Inc., Acerta Pharma, LLC, Deciphera Pharmaceuticals, LLC, Genentech, Inc., Roche Glycart AG, Syndax Pharmaceuticals Inc., Innate Pharma, and NanoString Technologies, and is a member of the Scientific Advisory Boards of Syndax Pharmaceuticals, Carisma Therapeutics, Zymeworks, Inc, Verseau Therapeutics, Cytomix Therapeutics, Inc., and Kineta Inc.
Figures
Comment in
-
Immunosurveillance and Regression in the Context of Squamous Pulmonary Premalignancy.Cancer Discov. 2020 Oct;10(10):1442-1444. doi: 10.1158/2159-8290.CD-20-1087. Cancer Discov. 2020. PMID: 33004476 Free PMC article.
References
-
- Nicholson AG, Perry LJ, Cury PM, Jackson P, McCormick CM, Corrin B, et al. Reproducibility of the WHO/IASLC grading system for pre-invasive squamous lesions of the bronchus: a study of inter-observer and intra-observer variation. Histopathology. 2001;38:202–8. - PubMed
-
- Mascaux C, Angelova M, Vasaturo A, Beane J, Hijazi K, Anthoine G, et al. Immune evasion before tumour invasion in early lung squamous carcinogenesis. Nature. 2019;571:570–5. - PubMed
Publication types
MeSH terms
Grants and funding
- U54 CA217376/CA/NCI NIH HHS/United States
- U01 CA224012/CA/NCI NIH HHS/United States
- R01 CA223150/CA/NCI NIH HHS/United States
- U2C CA233280/CA/NCI NIH HHS/United States
- 209199/WT_/Wellcome Trust/United Kingdom
- R01 CA226909/CA/NCI NIH HHS/United States
- 209199/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- 091730/WT_/Wellcome Trust/United Kingdom
- R21 HD099367/HD/NICHD NIH HHS/United States
- 835297/ERC_/European Research Council/International
- R01 CA185138/CA/NCI NIH HHS/United States
- 24956/CRUK_/Cancer Research UK/United Kingdom
- FC001169/CRUK_/Cancer Research UK/United Kingdom
- A11790/CRUK_/Cancer Research UK/United Kingdom
- 22246/CRUK_/Cancer Research UK/United Kingdom
- 20764/CRUK_/Cancer Research UK/United Kingdom
- 211179/Z/18/Z/WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
