

Image-based consensus molecular subtype (imCMS) classification of colorectal cancer using deep learning
- PMID: 32690604
- PMCID: PMC7873419
- DOI: 10.1136/gutjnl-2019-319866
Image-based consensus molecular subtype (imCMS) classification of colorectal cancer using deep learning
Abstract
Objective: Complex phenotypes captured on histological slides represent the biological processes at play in individual cancers, but the link to underlying molecular classification has not been clarified or systematised. In colorectal cancer (CRC), histological grading is a poor predictor of disease progression, and consensus molecular subtypes (CMSs) cannot be distinguished without gene expression profiling. We hypothesise that image analysis is a cost-effective tool to associate complex features of tissue organisation with molecular and outcome data and to resolve unclassifiable or heterogeneous cases. In this study, we present an image-based approach to predict CRC CMS from standard H&E sections using deep learning.
Design: Training and evaluation of a neural network were performed using a total of n=1206 tissue sections with comprehensive multi-omic data from three independent datasets (training on FOCUS trial, n=278 patients; test on rectal cancer biopsies, GRAMPIAN cohort, n=144 patients; and The Cancer Genome Atlas (TCGA), n=430 patients). Ground truth CMS calls were ascertained by matching random forest and single sample predictions from CMS classifier.
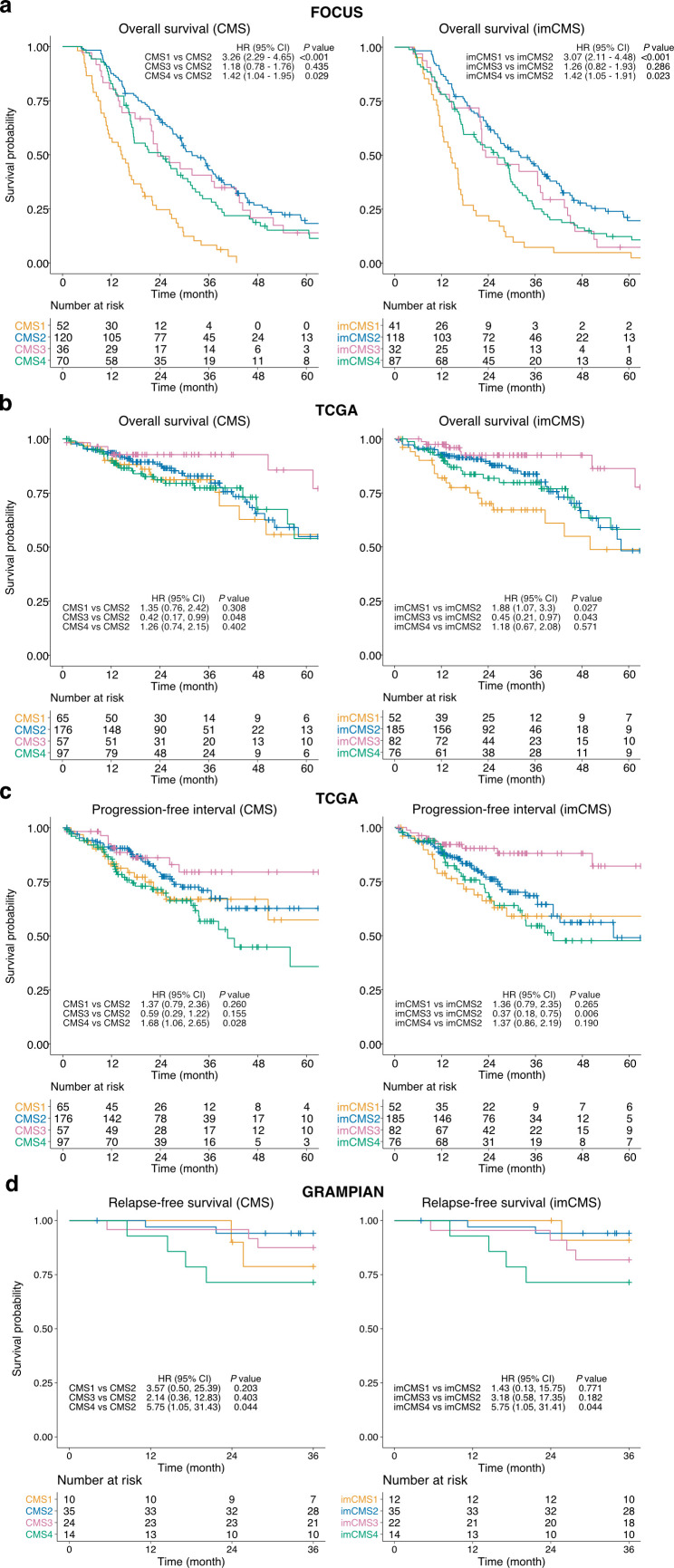
Results: Image-based CMS (imCMS) accurately classified slides in unseen datasets from TCGA (n=431 slides, AUC)=0.84) and rectal cancer biopsies (n=265 slides, AUC=0.85). imCMS spatially resolved intratumoural heterogeneity and provided secondary calls correlating with bioinformatic prediction from molecular data. imCMS classified samples previously unclassifiable by RNA expression profiling, reproduced the expected correlations with genomic and epigenetic alterations and showed similar prognostic associations as transcriptomic CMS.
Conclusion: This study shows that a prediction of RNA expression classifiers can be made from H&E images, opening the door to simple, cheap and reliable biological stratification within routine workflows.
Keywords: colorectal pathology; computerised image analysis; molecular pathology.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: KS and JR are co-founders of University of Oxford spinout Ground Truth Labs
Figures



References
-
- Sepulveda AR, Hamilton SR, Allegra CJ, et al. Molecular biomarkers for the evaluation of colorectal cancer: guideline from the American Society for clinical pathology, College of American pathologists, association for molecular pathology, and the American Society of clinical oncology. J Clin Oncol 2017;35:1453–86. 10.1200/JCO.2016.71.9807 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical