

Five years of ocrelizumab in relapsing multiple sclerosis: OPERA studies open-label extension
- PMID: 32690791
- PMCID: PMC7682822
- DOI: 10.1212/WNL.0000000000010376
Five years of ocrelizumab in relapsing multiple sclerosis: OPERA studies open-label extension
Abstract
Objective: To assess over 3 years of follow-up the effects of maintaining or switching to ocrelizumab (OCR) therapy on clinical and MRI outcomes and safety measures in the open-label extension (OLE) phase of the pooled OPERA: I/II studies in relapsing multiple sclerosis.
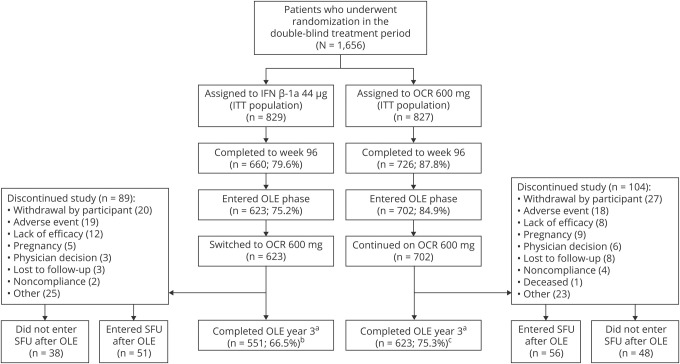
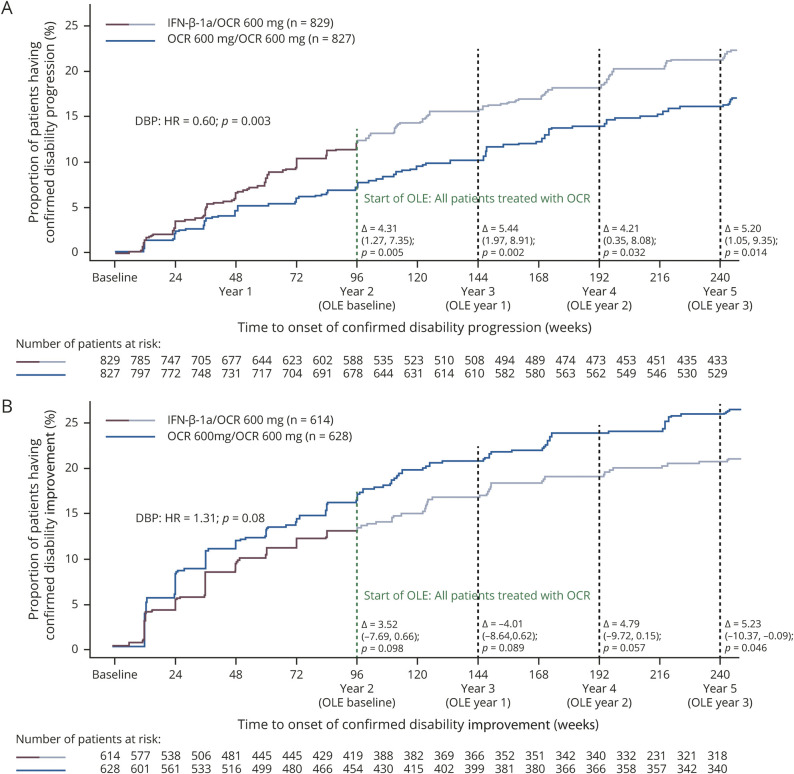
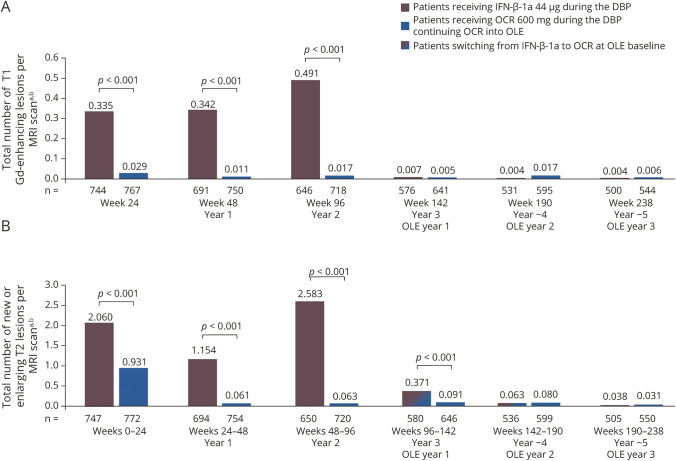
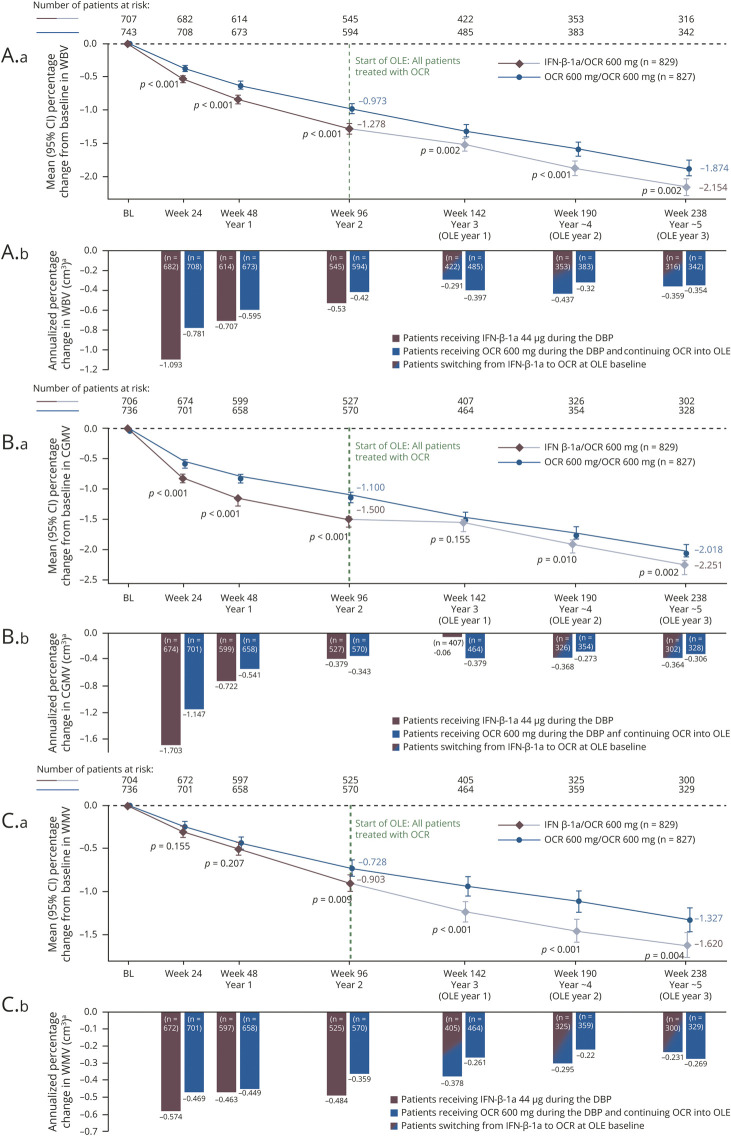
Methods: After 2 years of double-blind, controlled treatment, patients continued OCR (600 mg infusions every 24 weeks) or switched from interferon (IFN)-β-1a (44 μg 3 times weekly) to OCR when entering the OLE phase (3 years). Adjusted annualized relapse rate, time to onset of 24-week confirmed disability progression (CDP)/improvement (CDP), brain MRI activity (gadolinium-enhanced and new/enlarging T2 lesions), and percentage brain volume change were analyzed.
Results: Of patients entering the OLE phase, 88.6% completed year 5. The cumulative proportion with 24-week CDP was lower in patients who initiated OCR earlier vs patients initially receiving IFN-β-1a (16.1% vs 21.3% at year 5; p = 0.014). Patients continuing OCR maintained and those switching from IFN-β-1a to OCR attained near complete and sustained suppression of new brain MRI lesion activity from years 3-5. Over the OLE phase, patients continuing OCR exhibited less whole brain volume loss from double-blind study baseline vs those switching from IFN-β-1a (-1.87% vs -2.15% at year 5; p < 0.01). Adverse events were consistent with past reports and no new safety signals emerged with prolonged treatment.
Conclusion: Compared with patients switching from IFN-β-1a, earlier and continuous OCR treatment up to 5 years provided sustained benefit on clinical and MRI measures of disease progression.
Classification of evidence: This study provides Class III evidence that earlier and continuous treatment with OCR provided sustained benefit on clinical and MRI outcomes of disease activity and progression compared with patients switching from IFN-β-1a. The study is rated Class III because of the initial treatment randomization disclosure that occurred after inclusion in OLE.
Clinical trial identifiers: NCT01247324/NCT01412333.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures

References
-
- DiLillo DJ, Hamaguchi Y, Ueda Y, et al. Maintenance of long-lived plasma cells and serological memory despite mature and memory B cell depletion during CD20 immunotherapy in mice. J Immunol 2008;180:361–371. - PubMed
-
- Hauser SL, Bar-Or A, Comi G, et al. Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosis. N Engl J Med 2017;376:221–234. - PubMed
-
- Smith SM, Zhang Y, Jenkinson M, et al. Accurate, robust, and automated longitudinal and cross-sectional brain change analysis. Neuroimage 2002;17:479–489. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous