

Coronavirus infection (SARS-CoV-2) in obesity and diabetes comorbidities: is heat shock response determinant for the disease complications?
- PMID: 32690985
- PMCID: PMC7364287
- DOI: 10.1186/s13098-020-00572-w
Coronavirus infection (SARS-CoV-2) in obesity and diabetes comorbidities: is heat shock response determinant for the disease complications?
Abstract
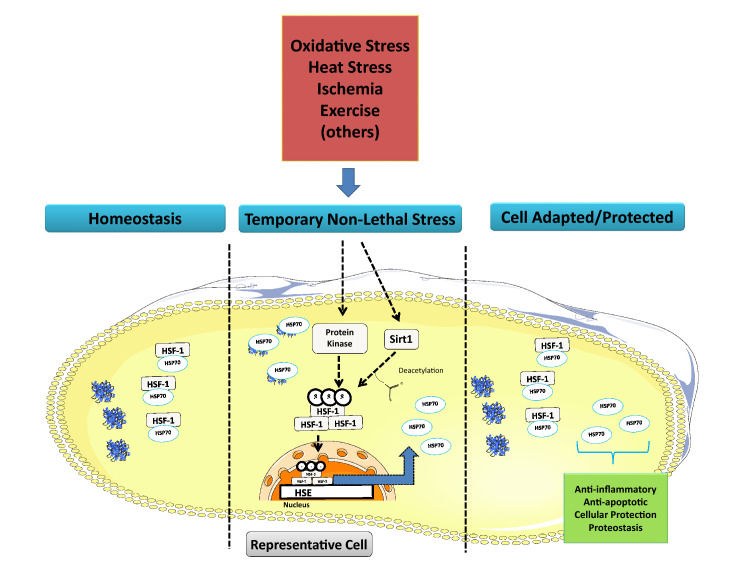
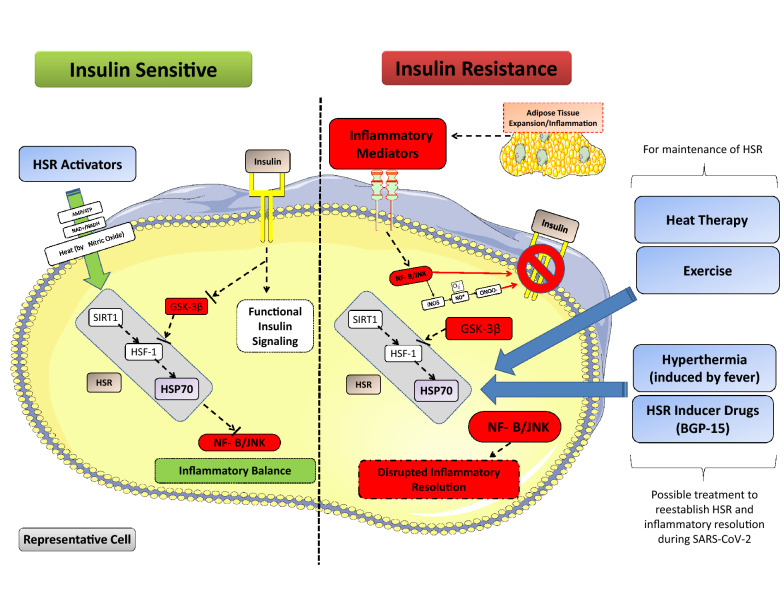
Chronic inflammation is involved in the pathogenesis of several metabolic diseases, such as obesity and type 2 diabetes mellitus (T2DM). With the recent worldwide outbreak of coronavirus disease (SARS-CoV-2), it has been observed that individuals with these metabolic diseases are more likely to develop complications, increasing the severity of the disease and a poorer outcome. Coronavirus infection leads to the activation of adaptive and innate immune responses, resulting in massive inflammation (to so called cytokine storm), which in turn can lead to damage to various tissues, septic shock and multiple organ failure. Recent evidence suggests that the common link between metabolic diseases and SARS-CoV-2 is the inflammatory response (chronic/low-grade for metabolic diseases and acute/intense in coronavirus infection). However, the ability of the infected individuals to resolve the inflammation has not yet been explored. The heat shock response (HSR), an important anti-inflammatory pathway, is reduced in patients with metabolic diseases and, consequently, may impair inflammation resolution and control in patients with SARS-CoV-2, thus enabling its amplification and propagation through all tissues. Herein, we present a new hypothesis that aims to explain the increased severity of SARS-CoV-2 infection in people with metabolic diseases, and the possible benefits of HSR-inducing therapies to improve the inflammatory profile in these patients.
Keywords: Heat shock response; Inflammation; Metabolic diseases; SARS-CoV-2.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsThe authors declare no competing interest as far as the contents of this manuscript are considered.
Figures

References
LinkOut - more resources
Full Text Sources
Miscellaneous
