

Evaluation of radixact motion synchrony for 3D respiratory motion: Modeling accuracy and dosimetric fidelity
- PMID: 32691973
- PMCID: PMC7497925
- DOI: 10.1002/acm2.12978
Evaluation of radixact motion synchrony for 3D respiratory motion: Modeling accuracy and dosimetric fidelity
Erratum in
-
Erratum: "Evaluation of radixact motion synchrony for 3D respiratory motion: Modeling accuracy and dosimetric fidelity".J Appl Clin Med Phys. 2023 Jan;24(1):e13805. doi: 10.1002/acm2.13805. J Appl Clin Med Phys. 2023. PMID: 36670523 Free PMC article. No abstract available.
Abstract
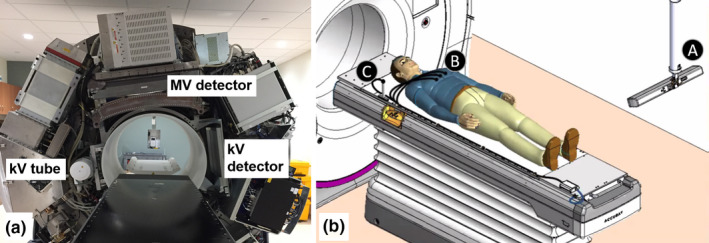
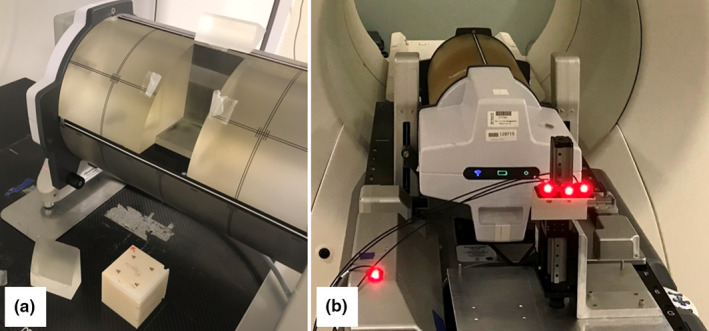
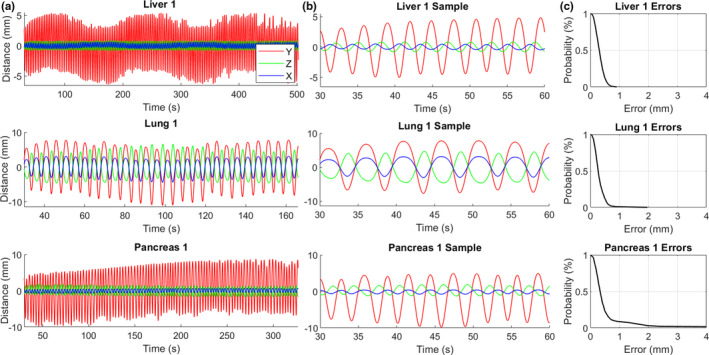
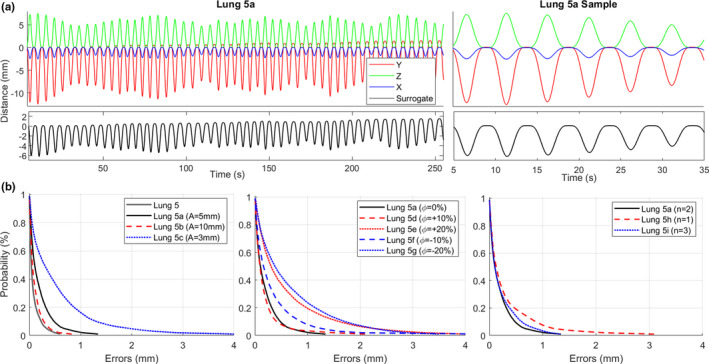
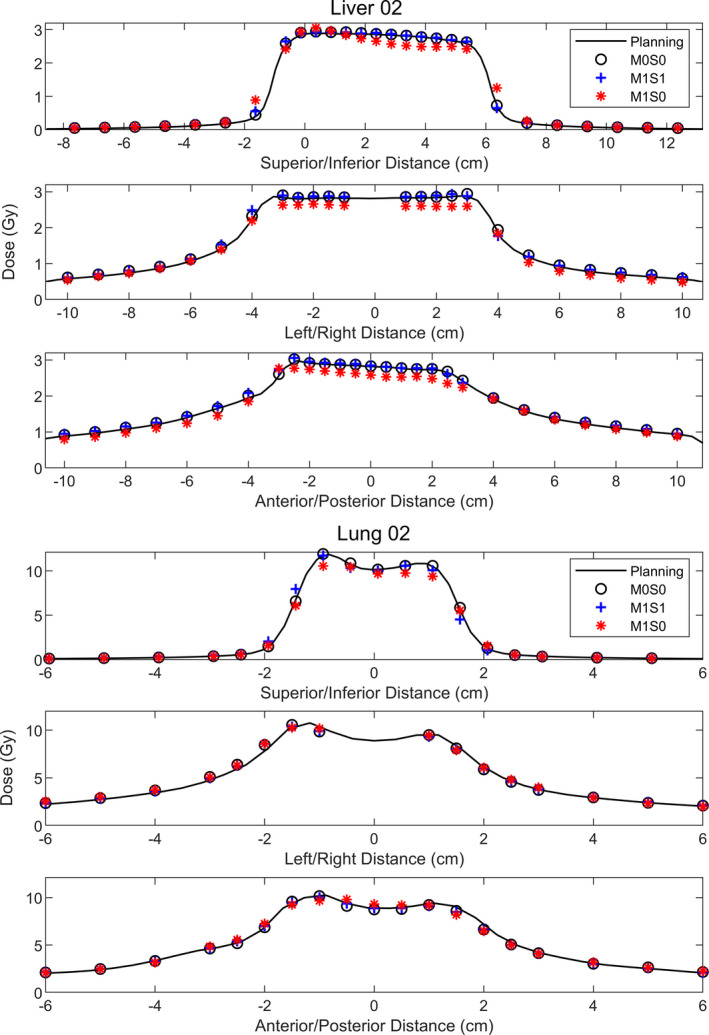
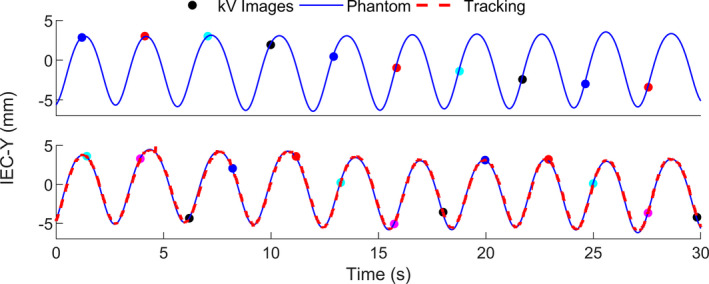
The Radixact® linear accelerator contains the motion Synchrony system, which tracks and compensates for intrafraction patient motion. For respiratory motion, the system models the motion of the target and synchronizes the delivery of radiation with this motion using the jaws and multi-leaf collimators (MLCs). It was the purpose of this work to determine the ability of the Synchrony system to track and compensate for different phantom motions using a delivery quality assurance (DQA) workflow. Thirteen helical plans were created on static datasets from liver, lung, and pancreas subjects. Dose distributions were measured using a Delta4® Phantom+ mounted on a Hexamotion® stage for the following three case scenarios for each plan: (a) no phantom motion and no Synchrony (M0S0), (b) phantom motion and no Synchrony (M1S0), and (c) phantom motion with Synchrony (M1S1). The LEDs were placed on the Phantom+ for the 13 patient cases and were placed on a separate one-dimensional surrogate stage for additional studies to investigate the effect of separate target and surrogate motion. The root-mean-square (RMS) error between the Synchrony-modeled positions and the programmed phantom positions was <1.5 mm for all Synchrony deliveries with the LEDs on the Phantom+. The tracking errors increased slightly when the LEDs were placed on the surrogate stage but were similar to tracking errors observed for other motion tracking systems such as CyberKnife Synchrony. One-dimensional profiles indicate the effects of motion interplay and dose blurring present in several of the M1S0 plans that are not present in the M1S1 plans. All 13 of the M1S1 measured doses had gamma pass rates (3%/2 mm/10%T) compared to the planned dose > 90%. Only two of the M1S0 measured doses had gamma pass rates > 90%. Motion Synchrony offers a potential alternative to the current, ITV-based motion management strategy for helical tomotherapy deliveries.
Keywords: intrafraction motion; radixact; synchrony; tomotherapy; tracking.
© 2020 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
Michael Kissick is an employed by and has ownership interests in Accuray Inc.
Figures
References
-
- Landberg T, Chavaudra J, Dobbs J, et al. Report 62: prescribing, recording, and reporting photon beam therapy (Supplement to ICRU Report 50). J ICRU. 1999;os32:NP.
-
- Bortfeld T, Jokivarsi K, Goitein M, Kung J, Jiang SB. Effects of intra‐fraction motion on IMRT dose delivery. Phys Med Biol. 2002;47:2203–2220. - PubMed
-
- Korreman SS. Motion in radiotherapy: photon therapy. Phys Med Biol. 2012;57:R161–R191. - PubMed
-
- Langen KM, Jones DTL. Organ motion and its management. Int J Radiat Oncol Biol Phys. 2001;50:265–278. - PubMed
-
- Keall PJ, Mageras GS, Balter JM, Emery RS, Forster KM, Jiang SB. The management of respiratory motion in radiation oncology report of AAPM Task Group 76. Med Phys. 2006;33:3874–3900. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
