

Impact of self-imposed prevention measures and short-term government-imposed social distancing on mitigating and delaying a COVID-19 epidemic: A modelling study
- PMID: 32692736
- PMCID: PMC7373263
- DOI: 10.1371/journal.pmed.1003166
Impact of self-imposed prevention measures and short-term government-imposed social distancing on mitigating and delaying a COVID-19 epidemic: A modelling study
Erratum in
-
Correction: Impact of self-imposed prevention measures and short-term government-imposed social distancing on mitigating and delaying a COVID-19 epidemic: A modelling study.PLoS Med. 2020 Dec 4;17(12):e1003499. doi: 10.1371/journal.pmed.1003499. eCollection 2020 Dec. PLoS Med. 2020. PMID: 33275595 Free PMC article.
Abstract
Background: The coronavirus disease (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has spread to nearly every country in the world since it first emerged in China in December 2019. Many countries have implemented social distancing as a measure to "flatten the curve" of the ongoing epidemics. Evaluation of the impact of government-imposed social distancing and of other measures to control further spread of COVID-19 is urgent, especially because of the large societal and economic impact of the former. The aim of this study was to compare the individual and combined effectiveness of self-imposed prevention measures and of short-term government-imposed social distancing in mitigating, delaying, or preventing a COVID-19 epidemic.
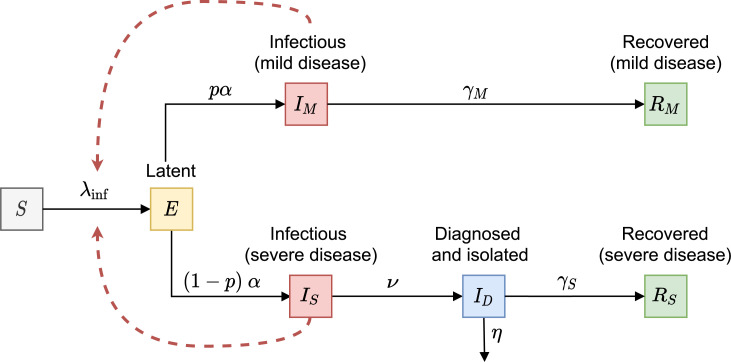
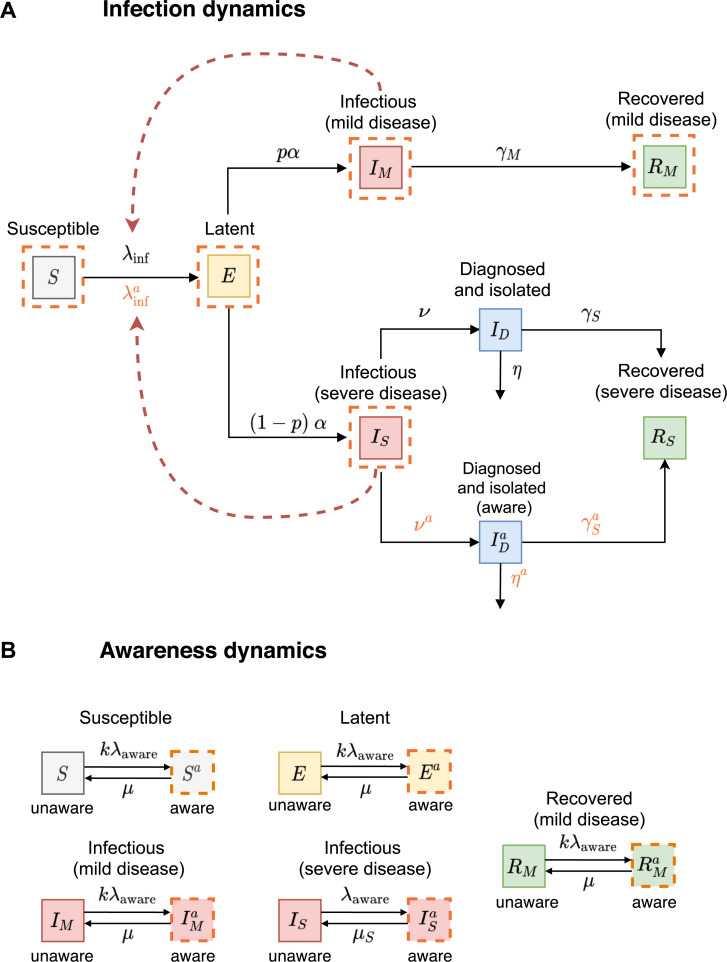
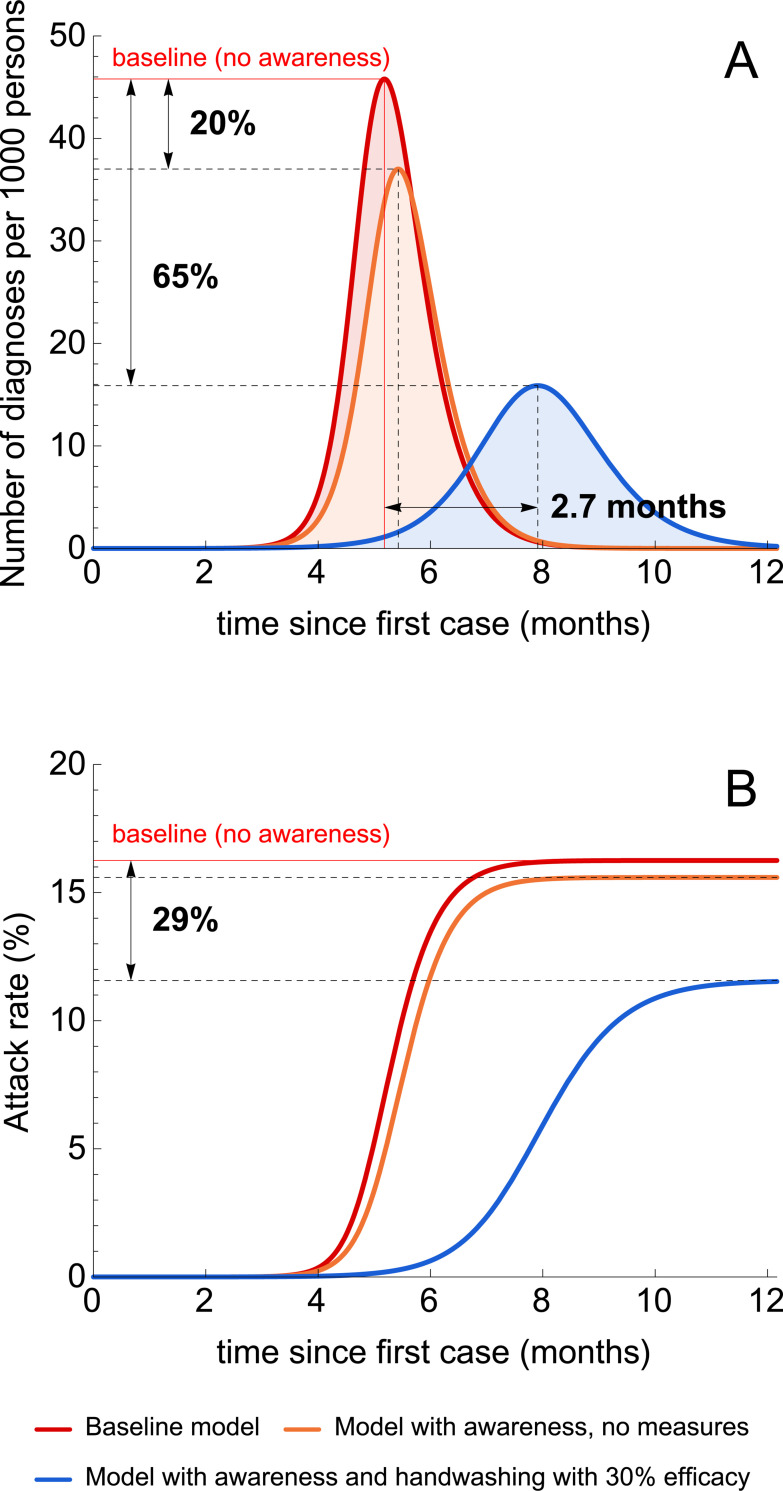
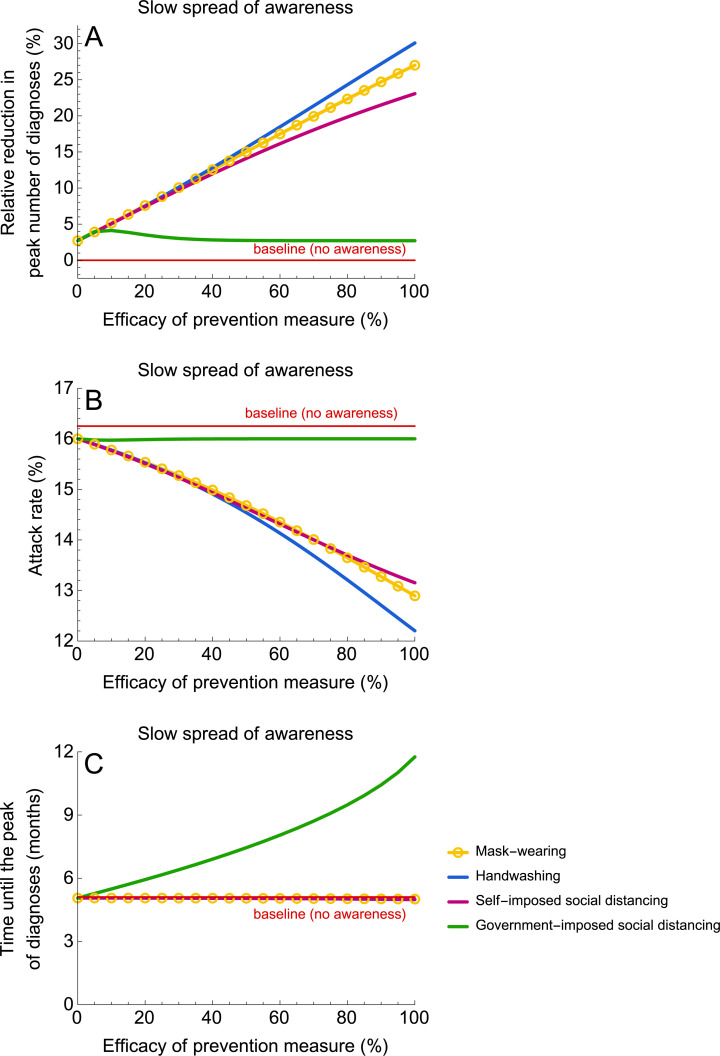
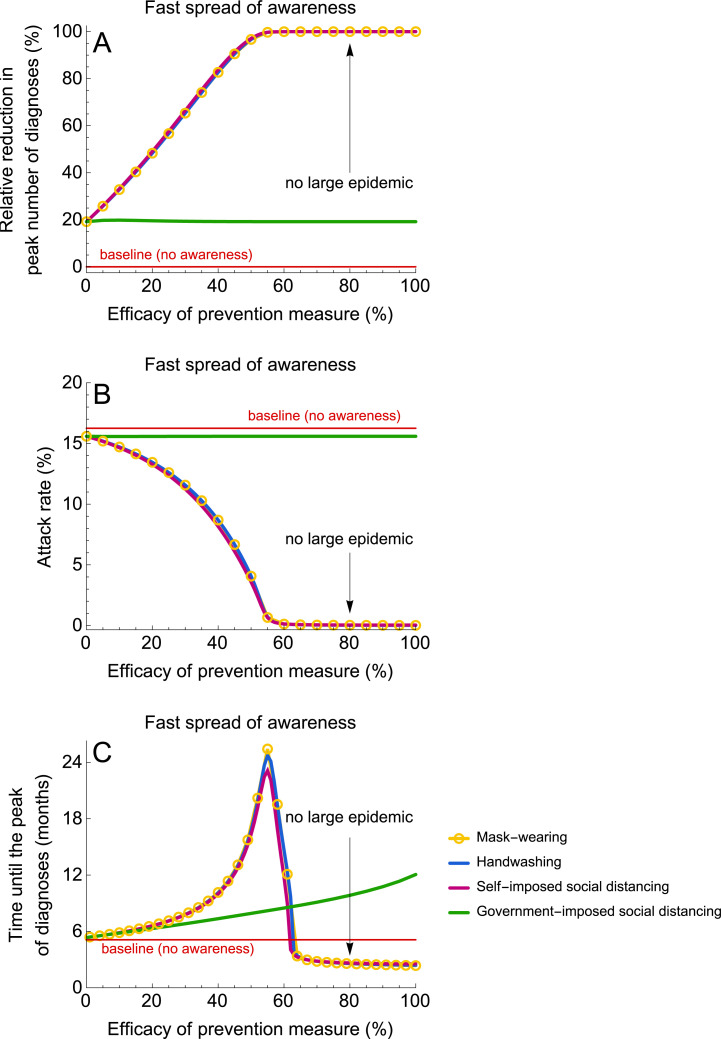
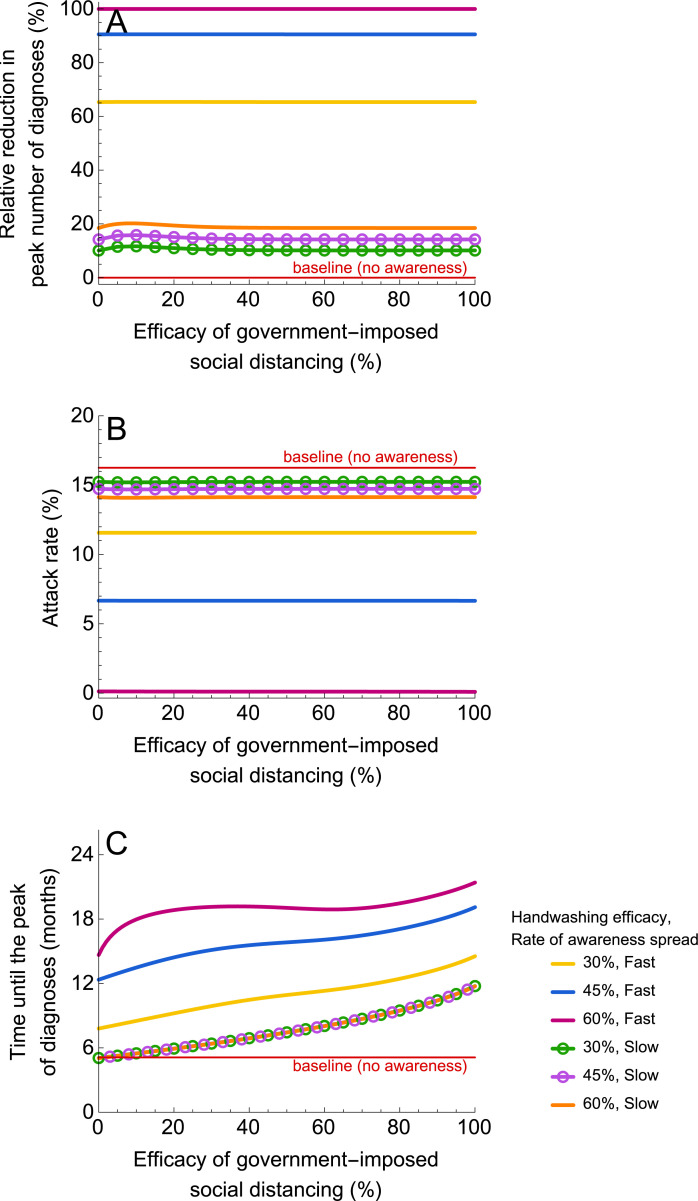
Methods and findings: We developed a deterministic compartmental transmission model of SARS-CoV-2 in a population stratified by disease status (susceptible, exposed, infectious with mild or severe disease, diagnosed, and recovered) and disease awareness status (aware and unaware) due to the spread of COVID-19. Self-imposed measures were assumed to be taken by disease-aware individuals and included handwashing, mask-wearing, and social distancing. Government-imposed social distancing reduced the contact rate of individuals irrespective of their disease or awareness status. The model was parameterized using current best estimates of key epidemiological parameters from COVID-19 clinical studies. The model outcomes included the peak number of diagnoses, attack rate, and time until the peak number of diagnoses. For fast awareness spread in the population, self-imposed measures can significantly reduce the attack rate and diminish and postpone the peak number of diagnoses. We estimate that a large epidemic can be prevented if the efficacy of these measures exceeds 50%. For slow awareness spread, self-imposed measures reduce the peak number of diagnoses and attack rate but do not affect the timing of the peak. Early implementation of short-term government-imposed social distancing alone is estimated to delay (by at most 7 months for a 3-month intervention) but not to reduce the peak. The delay can be even longer and the height of the peak can be additionally reduced if this intervention is combined with self-imposed measures that are continued after government-imposed social distancing has been lifted. Our analyses are limited in that they do not account for stochasticity, demographics, heterogeneities in contact patterns or mixing, spatial effects, imperfect isolation of individuals with severe disease, and reinfection with COVID-19.
Conclusions: Our results suggest that information dissemination about COVID-19, which causes individual adoption of handwashing, mask-wearing, and social distancing, can be an effective strategy to mitigate and delay the epidemic. Early initiated short-term government-imposed social distancing can buy time for healthcare systems to prepare for an increasing COVID-19 burden. We stress the importance of disease awareness in controlling the ongoing epidemic and recommend that, in addition to policies on social distancing, governments and public health institutions mobilize people to adopt self-imposed measures with proven efficacy in order to successfully tackle COVID-19.
Conflict of interest statement
MEK is a member of the Editorial Board of PLOS Medicine. The authors have declared that no competing interests exist.
Figures
Comment in
-
Can self-imposed prevention measures mitigate the COVID-19 epidemic?PLoS Med. 2020 Jul 21;17(7):e1003240. doi: 10.1371/journal.pmed.1003240. eCollection 2020 Jul. PLoS Med. 2020. PMID: 32692743 Free PMC article.
References
-
- World Health Organization. Coronavirus disease 2019 (COVID-19). Situation Report–51; 2020 March 11. [cited 2020 Mar 13]. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/2....
-
- Tindale L, Coombe M, Stockdale JE, Garlock E, Lau WYV, Saraswat M, et al. Transmission interval estimates suggest pre-symptomatic spread of COVID-19. medRxiv:2020.03.03.20029983 [Preprint]. 2020. [cited 2020 Jun 25]. https://www.medrxiv.org/content/10.1101/2020.03.03.20029983v1 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
