

A Phase Ib/IIa Study of the Pan-BET Inhibitor ZEN-3694 in Combination with Enzalutamide in Patients with Metastatic Castration-resistant Prostate Cancer
- PMID: 32694156
- PMCID: PMC7572827
- DOI: 10.1158/1078-0432.CCR-20-1707
A Phase Ib/IIa Study of the Pan-BET Inhibitor ZEN-3694 in Combination with Enzalutamide in Patients with Metastatic Castration-resistant Prostate Cancer
Abstract
Purpose: ZEN-3694 is a bromodomain extraterminal inhibitor (BETi) with activity in androgen-signaling inhibitor (ASI)-resistant models. The safety and efficacy of ZEN-3694 plus enzalutamide was evaluated in a phase Ib/IIa study in metastatic castration-resistant prostate cancer (mCRPC).
Patients and methods: Patients had progressive mCRPC with prior resistance to abiraterone and/or enzalutamide. 3+3 dose escalation was followed by dose expansion in parallel cohorts (ZEN-3694 at 48 and 96 mg orally once daily, respectively).
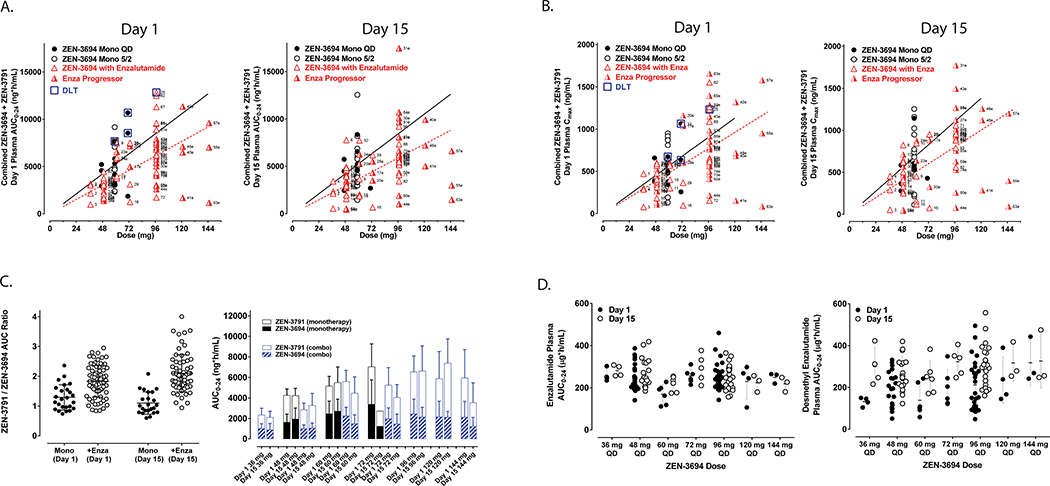
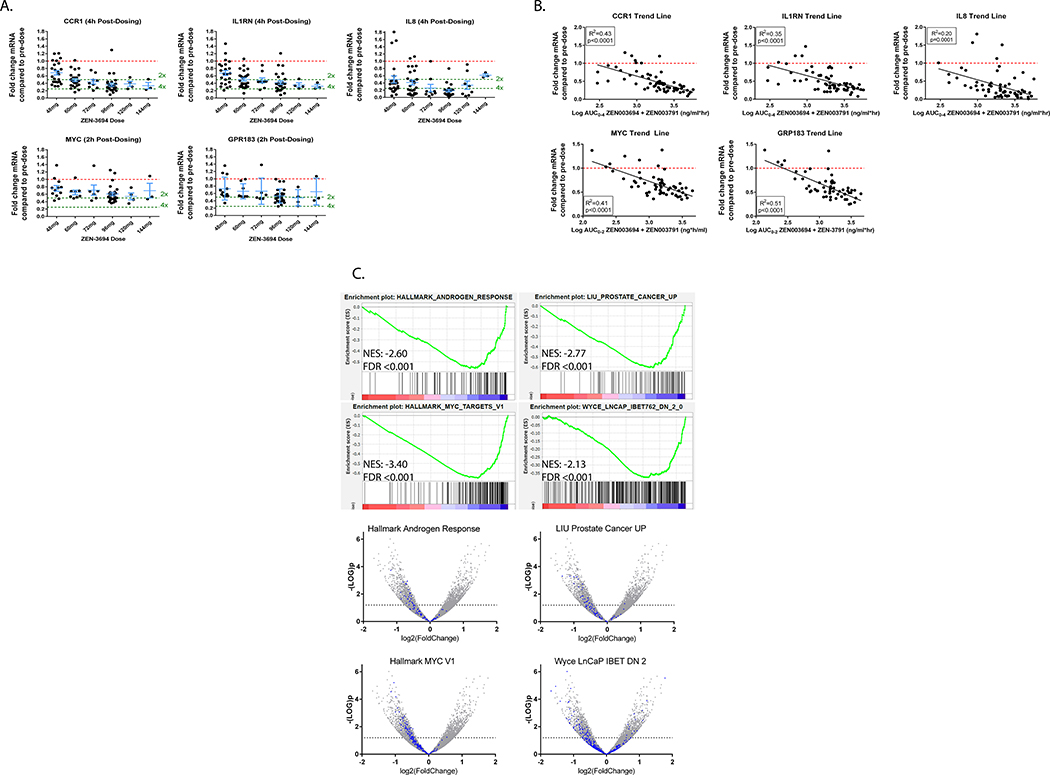
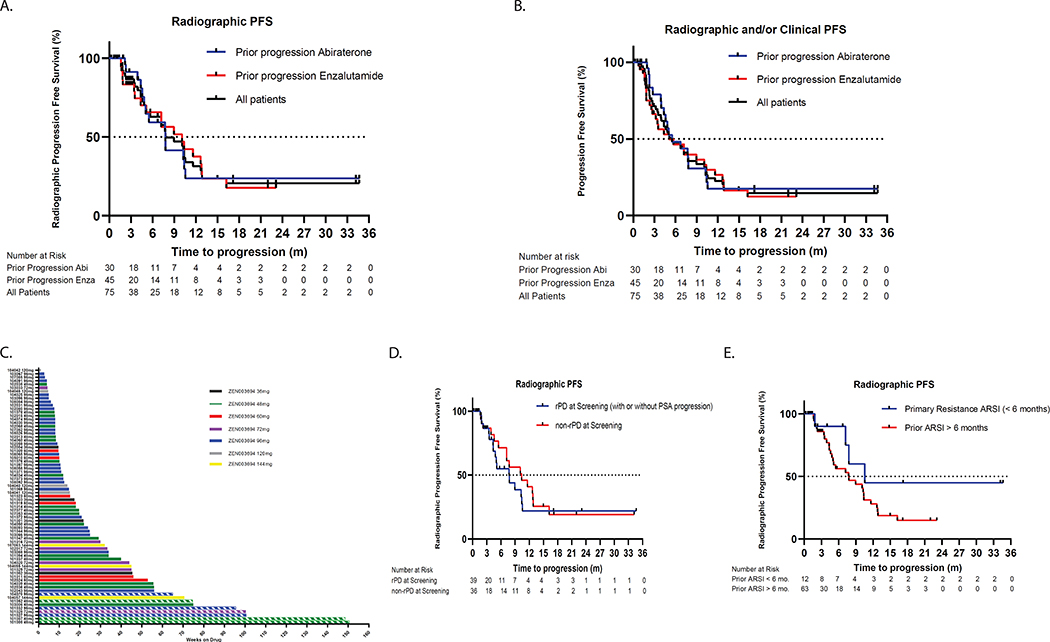
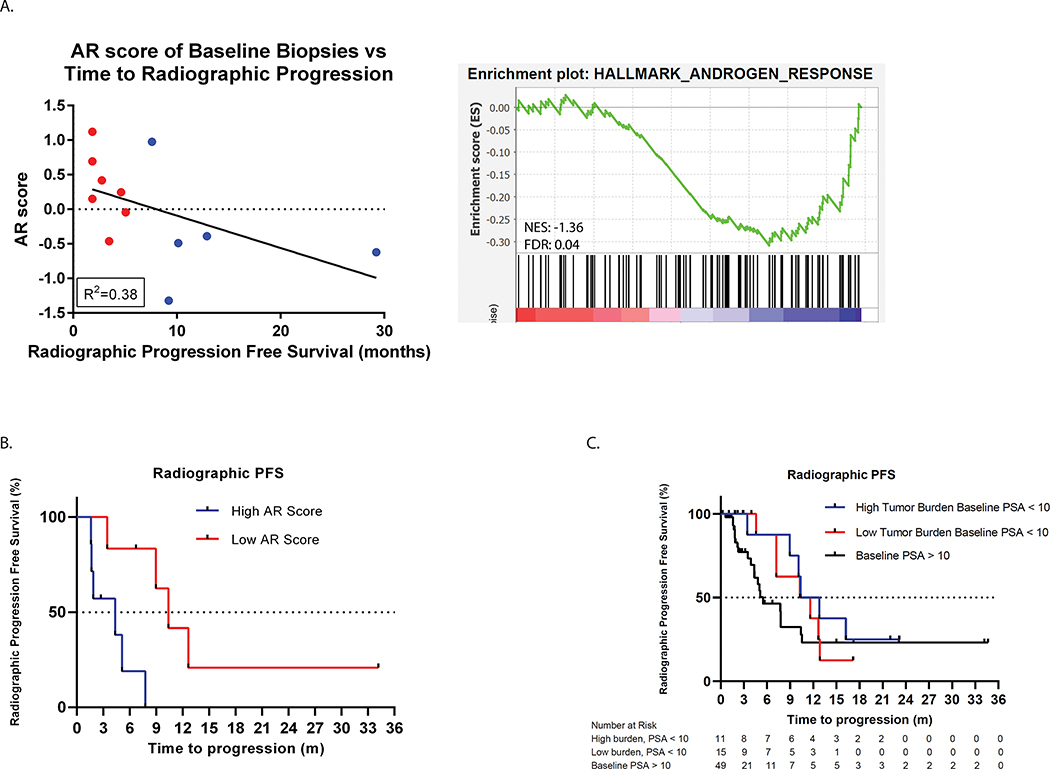
Results: Seventy-five patients were enrolled (N = 26 and 14 in dose expansion at low- and high-dose ZEN-3694, respectively). Thirty (40.0%) patients were resistant to abiraterone, 34 (45.3%) to enzalutamide, and 11 (14.7%) to both. ZEN-3694 dosing ranged from 36 to 144 mg daily without reaching an MTD. Fourteen patients (18.7%) experienced grade ≥3 toxicities, including three patients with grade 3 thrombocytopenia (4%). An exposure-dependent decrease in whole-blood RNA expression of BETi targets was observed (up to fourfold mean difference at 4 hours post-ZEN-3694 dose; P ≤ 0.0001). The median radiographic progression-free survival (rPFS) was 9.0 months [95% confidence interval (CI), 4.6-12.9] and composite median radiographic or clinical progression-free survival (PFS) was 5.5 months (95% CI, 4.0-7.8). Median duration of treatment was 3.5 months (range, 0-34.7+). Lower androgen receptor (AR) transcriptional activity in baseline tumor biopsies was associated with longer rPFS (median rPFS 10.4 vs. 4.3 months).
Conclusions: ZEN-3694 plus enzalutamide demonstrated acceptable tolerability and potential efficacy in patients with ASI-resistant mCRPC. Further prospective study is warranted including in mCRPC harboring low AR transcriptional activity.
©2020 American Association for Cancer Research.
Figures
Similar articles
-
Plasma Androgen Receptor and Docetaxel for Metastatic Castration-resistant Prostate Cancer.Eur Urol. 2019 Mar;75(3):368-373. doi: 10.1016/j.eururo.2018.09.049. Epub 2018 Oct 26. Eur Urol. 2019. PMID: 30773204 Free PMC article.
-
Effectiveness of first-line abiraterone versus enzalutamide among patients ≥80 years of age with metastatic castration-resistant prostate cancer: A retrospective propensity score-weighted comparative cohort study.Eur J Cancer. 2021 Jul;152:215-222. doi: 10.1016/j.ejca.2021.05.003. Epub 2021 Jun 12. Eur J Cancer. 2021. PMID: 34130153
-
Comparison of effectiveness and safety outcomes of abiraterone versus enzalutamide in patients with metastatic castration-resistant prostate cancer: a systematic review and meta-analysis.J Pharm Pharm Sci. 2020;23:451-461. doi: 10.18433/jpps31003. J Pharm Pharm Sci. 2020. PMID: 33217255
-
Efficacy and Safety of Cabazitaxel Versus Abiraterone or Enzalutamide in Older Patients with Metastatic Castration-resistant Prostate Cancer in the CARD Study.Eur Urol. 2021 Oct;80(4):497-506. doi: 10.1016/j.eururo.2021.06.021. Epub 2021 Jul 15. Eur Urol. 2021. PMID: 34274136 Clinical Trial.
-
What do we know about treatment sequencing of abiraterone, enzalutamide, and chemotherapy in metastatic castration-resistant prostate cancer?World J Urol. 2016 May;34(5):617-24. doi: 10.1007/s00345-015-1687-0. Epub 2015 Sep 15. World J Urol. 2016. PMID: 26373956
Cited by
-
Understanding the Roles of the NSD Protein Methyltransferases in Head and Neck Squamous Cell Carcinoma.Genes (Basel). 2022 Nov 2;13(11):2013. doi: 10.3390/genes13112013. Genes (Basel). 2022. PMID: 36360250 Free PMC article. Review.
-
Selectivity Mechanism of Pyrrolopyridone Analogues Targeting Bromodomain 2 of Bromodomain-Containing Protein 4 from Molecular Dynamics Simulations.ACS Omega. 2023 Sep 6;8(37):33658-33674. doi: 10.1021/acsomega.3c03935. eCollection 2023 Sep 19. ACS Omega. 2023. PMID: 37744850 Free PMC article.
-
BET Bromodomain Inhibition Blocks an AR-Repressed, E2F1-Activated Treatment-Emergent Neuroendocrine Prostate Cancer Lineage Plasticity Program.Clin Cancer Res. 2021 Sep 1;27(17):4923-4936. doi: 10.1158/1078-0432.CCR-20-4968. Epub 2021 Jun 18. Clin Cancer Res. 2021. PMID: 34145028 Free PMC article.
-
Molecular Mechanisms of Prostate Cancer Development in the Precision Medicine Era: A Comprehensive Review.Cancers (Basel). 2024 Jan 25;16(3):523. doi: 10.3390/cancers16030523. Cancers (Basel). 2024. PMID: 38339274 Free PMC article. Review.
-
Epigenetic (De)regulation in Prostate Cancer.Cancer Treat Res. 2023;190:321-360. doi: 10.1007/978-3-031-45654-1_10. Cancer Treat Res. 2023. PMID: 38113006 Free PMC article.
References
-
- Siegel RL, Miller KD, and Jemal A. Cancer statistics, 2020. CA: A Cancer Journal for Clinicians 2020;70(1):7–30. - PubMed
-
- Fizazi K, Tran N, Fein L, et al. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncology 2019;20:686–70. - PubMed
-
- Chi KN, Agarwal N, Anders B, et al. Apalutamide for metastatic castation-sensitive prostate cancer. New Engl J Med 2019:381:13–24. - PubMed
