

Identification of a unique temporal signature in blood and BAL associated with IPF progression
- PMID: 32694604
- PMCID: PMC7374599
- DOI: 10.1038/s41598-020-67956-w
Identification of a unique temporal signature in blood and BAL associated with IPF progression
Abstract
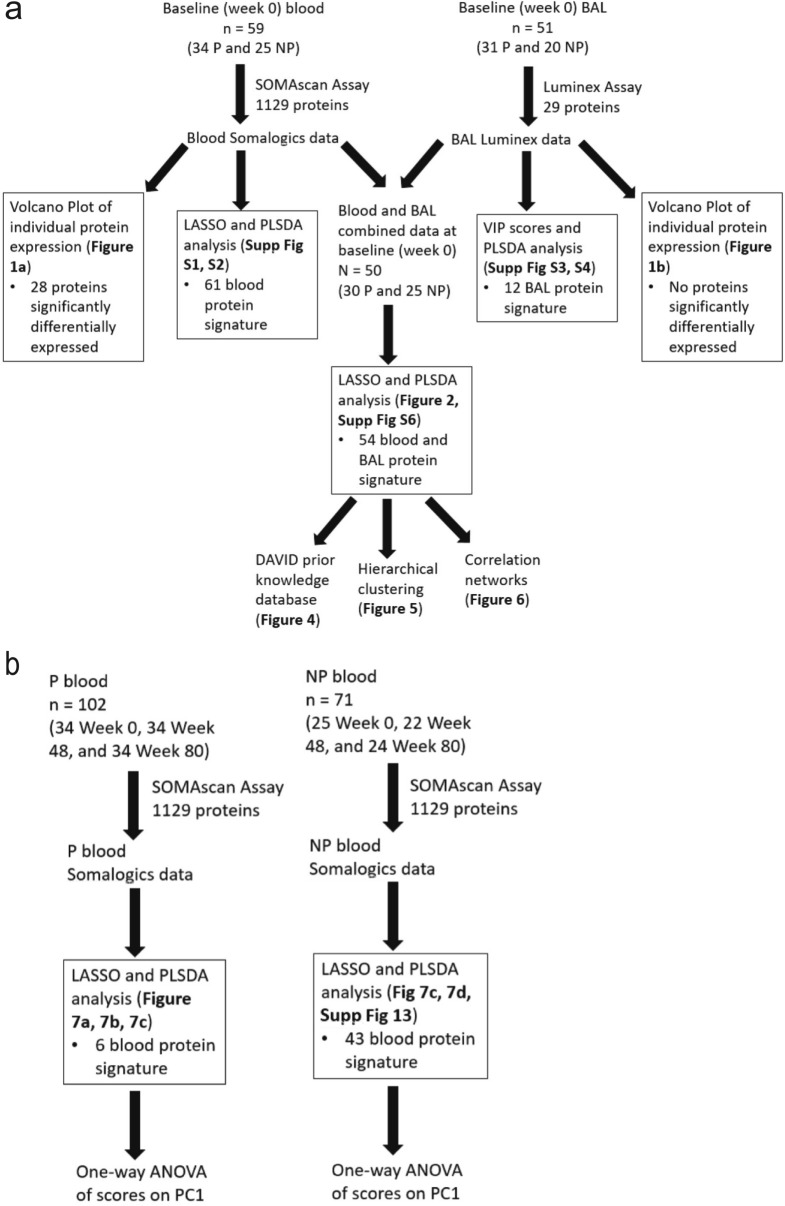
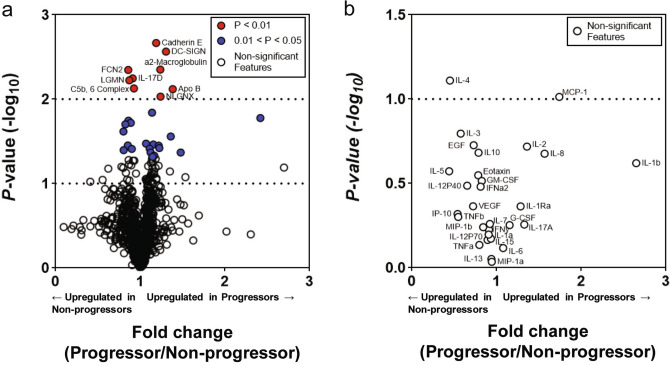
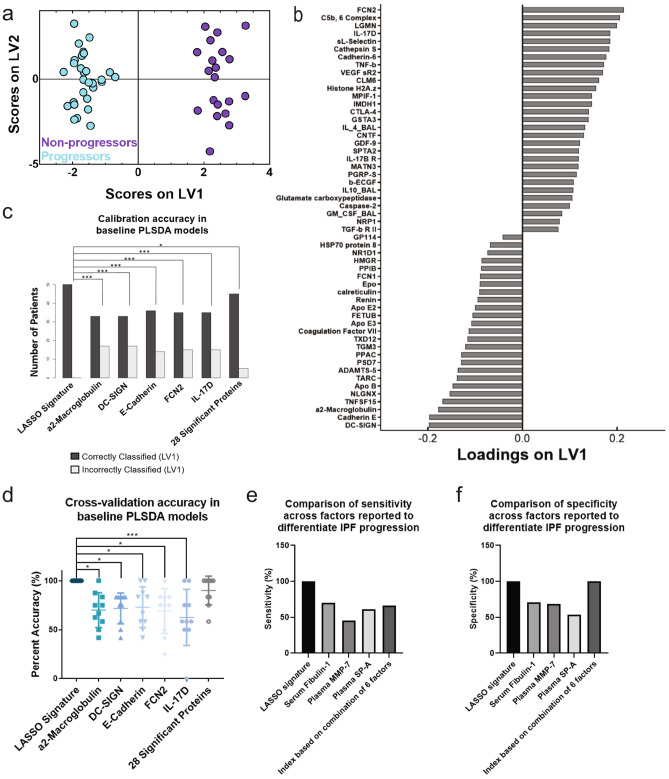
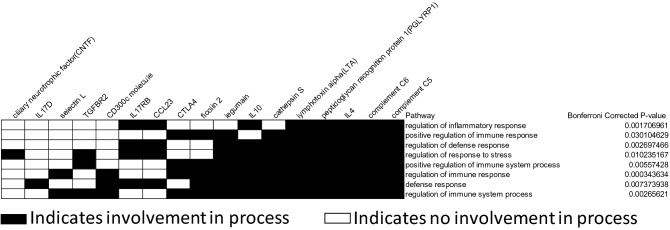
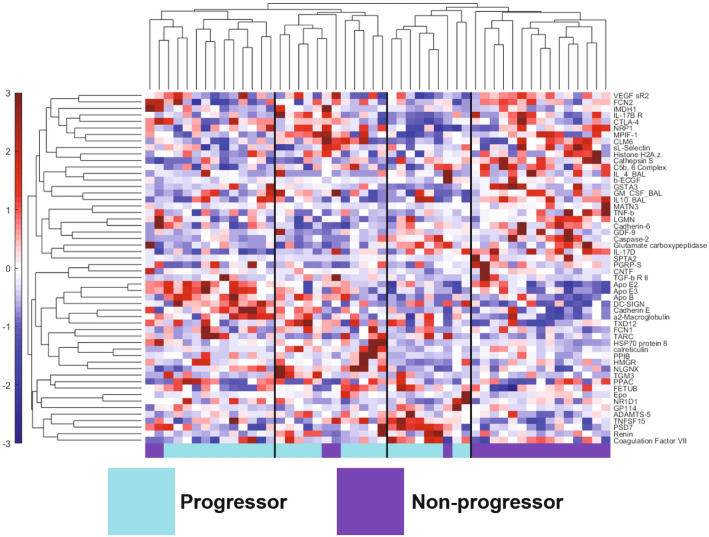
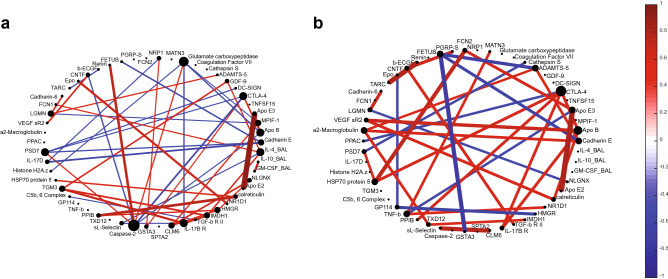
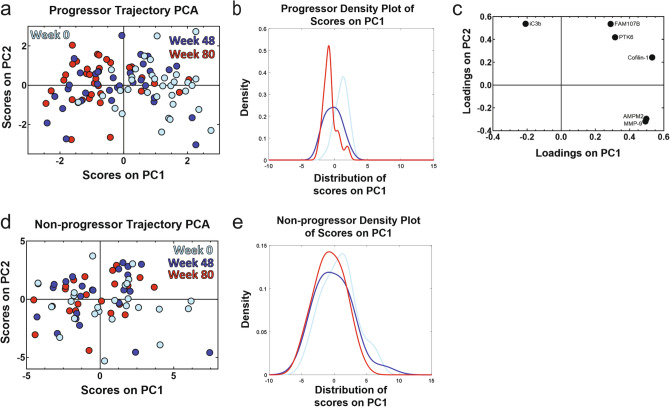
Idiopathic pulmonary fibrosis (IPF) is a progressive and heterogeneous interstitial lung disease of unknown origin with a low survival rate. There are few treatment options available due to the fact that mechanisms underlying disease progression are not well understood, likely because they arise from dysregulation of complex signaling networks spanning multiple tissue compartments. To better characterize these networks, we used systems-focused data-driven modeling approaches to identify cross-tissue compartment (blood and bronchoalveolar lavage) and temporal proteomic signatures that differentiated IPF progressors and non-progressors. Partial least squares discriminant analysis identified a signature of 54 baseline (week 0) blood and lung proteins that differentiated IPF progression status by the end of 80 weeks of follow-up with 100% cross-validation accuracy. Overall we observed heterogeneous protein expression patterns in progressors compared to more homogenous signatures in non-progressors, and found that non-progressors were enriched for proteomic processes involving regulation of the immune/defense response. We also identified a temporal signature of blood proteins that was significantly different at early and late progressor time points (p < 0.0001), but not present in non-progressors. Overall, this approach can be used to generate new hypothesis for mechanisms associated with IPF progression and could readily be translated to other complex and heterogeneous diseases.
Conflict of interest statement
K.C.N., D.N.O., K.M.D., V.N.L., M.X., S.J.G, E.S.W., S.M., B.B.M., and K.B.A. report no competing interests. M.L.S. reports compensation for participation on a scientific advisory board, speaking, and consultancy for Boehringer Ingelheim Pharmaceuticals, Inc, unrelated to this manuscript. K.R.F. reports grants and consulting fees from Boehringer Ingelheim, grants and consulting fees from Roche/Genentech, and consulting fees from Veracyte, Fibrogen, Sanofi-Genzyme, and Celgene, outside of this project. F.J.M. has received personal fees from Forest, Janssen, GlaxoSmithKline, Nycomed/Takeda, Amgen, AstraZeneca, Boehringer Ingelheim, Ikaria/Bellerophon, Genentech, Novartis, Pearl, Pfizer, Roche, Sunovion, Theravance, Axon, CME Incite, California Society for Allergy and Immunology, Annenberg, Integritas, InThough, Miller Medical, National Association for Continuing Education, Paradigm, Peer Voice, UpToDate, Haymarket Communications, Western Society of Allergy and Immunology, Informa, Bioscale, Unity Biotechnology, ConCert, Lucid, Methodist Hospital, Prime, WebMD, Bayer, Ikaria, Kadmon, Vercyte, American Thoracic Society, Academic CME, Falco, Axon Communication, Johnson & Johnson, Clarion, Continuing Education, Potomac, Afferent, and Adept; and has collected nonfinancial support from Boehringer Ingelheim, Centocor, Gilead, and Biogen/Stromedix; and declares other interests with Mereo, Boehringering Ingelheim, and Centocor. All are outside of this project.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
