

Diagnostic efficacy of 2-shot compressed sensing cine sequence cardiovascular magnetic resonance imaging for left ventricular function
- PMID: 32695623
- PMCID: PMC7369273
- DOI: 10.21037/cdt-20-135
Diagnostic efficacy of 2-shot compressed sensing cine sequence cardiovascular magnetic resonance imaging for left ventricular function
Abstract
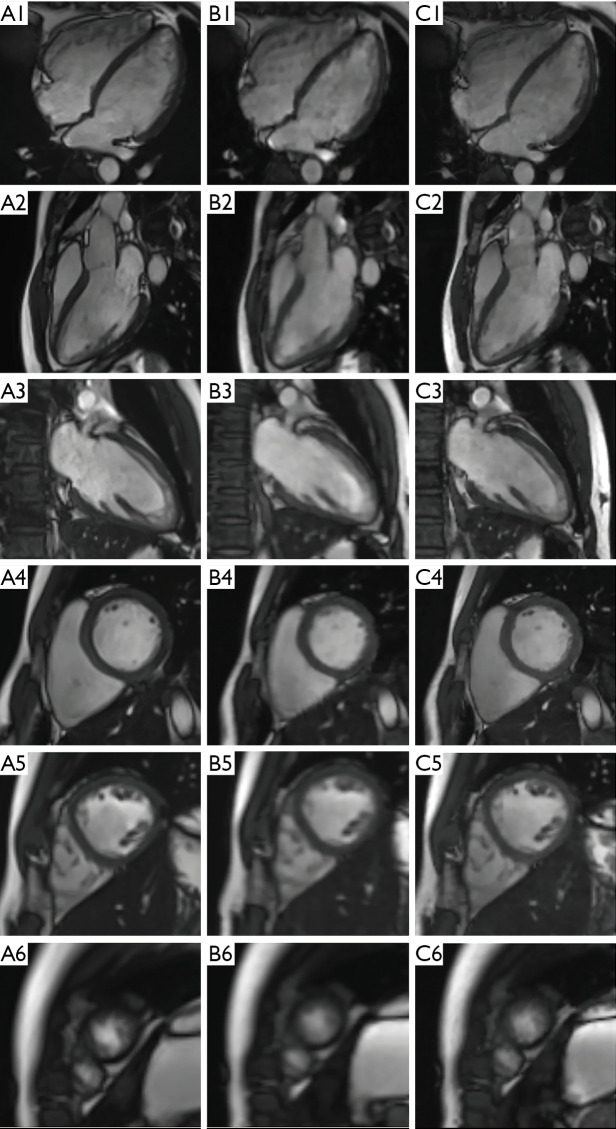
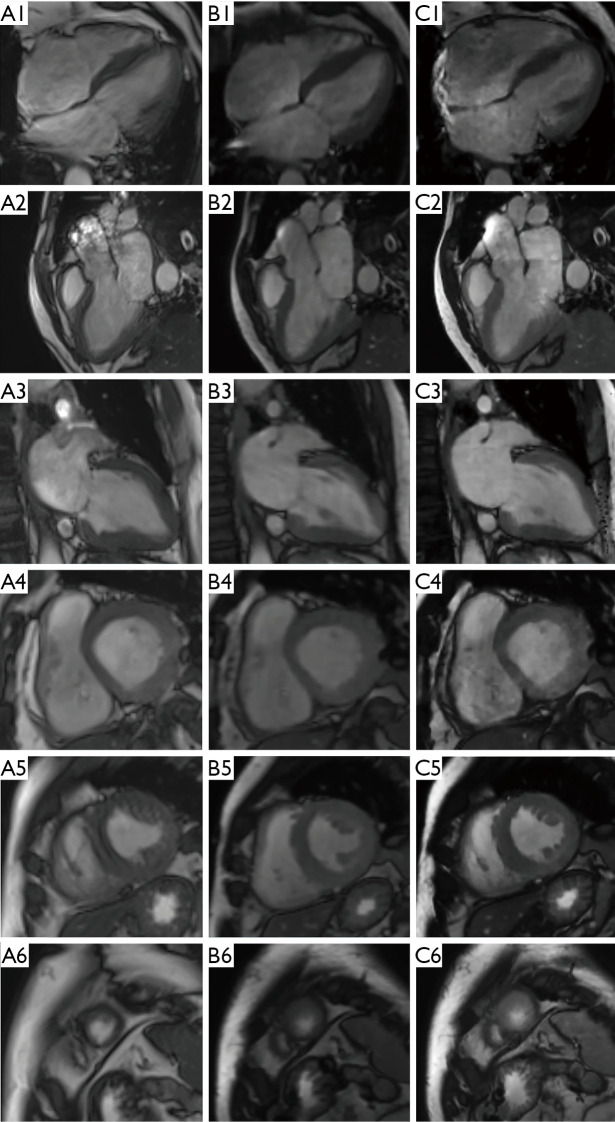
Background: Cardiac magnetic resonance cine images are conventionally acquired in breath-hold with a segmented balanced steady-state free precession (bSSFP) sequence, which requires a relatively long acquisition time and high patient cooperation. The single-shot compressed sensing (ss CS) cine sequence is a real-time sequence that has reasonable spatial and temporal resolution and can be applied during free breathing. However, the contrast between the myocardium and surrounding soft tissue is relatively reduced, and the epicardial delineation results are not as accurate with the ss CS cine sequence compared with the bSSFP sequence. In this study, we evaluated the use of a 2-shot CS cine technique in quickly acquiring high-quality images and accurately assessing cardiac function in clinical practice.
Methods: The patients enrolled in the study underwent cardiovascular magnetic resonance (CMR) on a 3T scanner from Jul. to Dec. 2018. Cine imaging was performed with 3 different methods: a standard segment cine sequence, a real-time ss CS cine sequence, and a 2-shot CS cine sequence prototype. Quantitative analysis of image quality was performed using a 0-4 scoring system, and also edge sharpness was measured, and cardiac function analysis was performed for all 3 types of cine images.
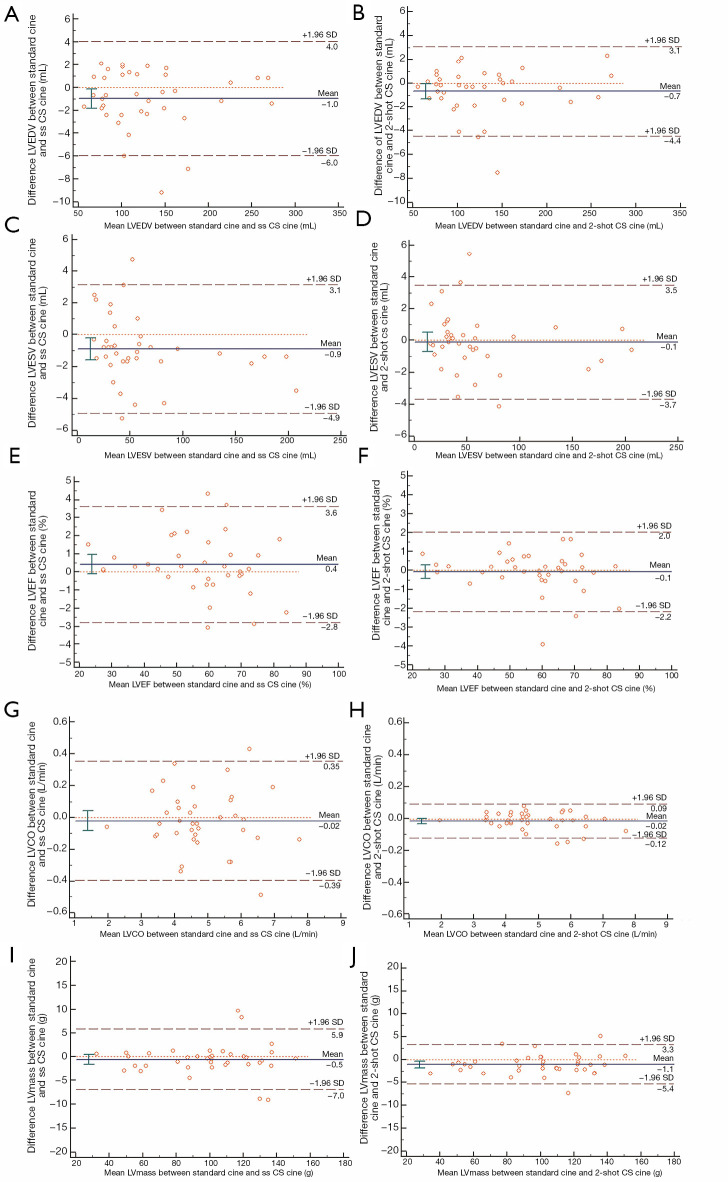
Results: Thirty-eight patients underwent imaging with the three types of cine sequences. The average scan time of the standard cine sequence was 101±20 s, the average scan time of the ss CS cine sequence was 20±4 s, and the average scan time of the 2-shot CS cine sequence was 30±6 s. The standard cine sequence image score was 3.68±0.64 and edge sharpness was (2.47±0.18) mm, the ss CS cine sequence image score was 3.13±0.35 and edge sharpness was (4.69±0.02) mm, and the 2-shot cine sequence image score was 3.54±0.51 and the edge sharpness was (2.51±0.13) mm. In terms of the quantitative study of cardiac function, the differences between the standard cine sequence and the ss CS cine sequence were not statistically significant, except for those of the imaging score and LV mass. There were no significant differences in the cardiac function parameters between the standard cine sequence and the 2-shot cine sequence. There was a strong correlation between the standard cine and ss CS cine sequences and between the standard cine and 2-shot CS cine sequences (P<0.01) of all the cardiac function parameters.
Conclusions: The 2-shot CS cine sequence can acquire images with a level of quality comparable to that of the standard cine sequence in a significantly shorter period of time. The functional parameters are similar between the 2-shot CS cine sequence and the standard cine sequence.
Keywords: Compressed sensing (CS); cardiovascular magnetic resonance (CMR) imaging; cine.
2020 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at: http://dx.doi.org/10.21037/cdt-20-135). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Utility of single-shot compressed sensing cardiac magnetic resonance cine imaging for assessment of biventricular function in free-breathing and arrhythmic pediatric patients.Int J Cardiol. 2021 Sep 1;338:258-264. doi: 10.1016/j.ijcard.2021.06.043. Epub 2021 Jun 26. Int J Cardiol. 2021. PMID: 34181995
-
Compressed sensing real-time cine cardiovascular magnetic resonance: accurate assessment of left ventricular function in a single-breath-hold.J Cardiovasc Magn Reson. 2016 Aug 24;18(1):50. doi: 10.1186/s12968-016-0271-0. J Cardiovasc Magn Reson. 2016. PMID: 27553656 Free PMC article.
-
Cardiac compressed sensing real-time cine for the assessment of left ventricular function: a large sample size analysis.Quant Imaging Med Surg. 2024 Dec 5;14(12):8785-8797. doi: 10.21037/qims-24-980. Epub 2024 Nov 29. Quant Imaging Med Surg. 2024. PMID: 39698697 Free PMC article.
-
[Feasibility of Single-Breath-Hold Compressed Sensing Real-Time Cine Imaging for Assessment of Ventricular Function and Left Ventricular Strain in Cardiac Magnetic Resonance].Sichuan Da Xue Xue Bao Yi Xue Ban. 2022 May;53(3):497-503. doi: 10.12182/20220560506. Sichuan Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 35642161 Free PMC article. Chinese.
-
Higher resolution cine imaging with compressed sensing for accelerated clinical left ventricular evaluation.J Magn Reson Imaging. 2017 Jun;45(6):1693-1699. doi: 10.1002/jmri.25525. Epub 2016 Oct 26. J Magn Reson Imaging. 2017. PMID: 27783472
Cited by
-
Right Ventricular Volume and Function Assessment in Congenital Heart Disease Using CMR Compressed-Sensing Real-Time Cine Imaging.J Clin Med. 2021 Apr 29;10(9):1930. doi: 10.3390/jcm10091930. J Clin Med. 2021. PMID: 33947025 Free PMC article.
-
Comparison of right atrial volume measurements using single-plane area-length and stack-of-short-axis methods: A 3.0 T cardiac magnetic resonance study.BMC Med Imaging. 2025 May 14;25(1):160. doi: 10.1186/s12880-025-01708-y. BMC Med Imaging. 2025. PMID: 40369433 Free PMC article.
-
Comparison between compressed sensing and segmented cine cardiac magnetic resonance: a meta-analysis.BMC Cardiovasc Disord. 2023 Sep 21;23(1):473. doi: 10.1186/s12872-023-03426-1. BMC Cardiovasc Disord. 2023. PMID: 37735355 Free PMC article.
-
Feasibility of one breath-hold cardiovascular magnetic resonance compressed sensing cine for left ventricular strain analysis.Front Cardiovasc Med. 2022 Aug 12;9:903203. doi: 10.3389/fcvm.2022.903203. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36035944 Free PMC article.
-
Optimizing Clinical Cardiac MRI Workflow through Single Breath-Hold Compressed Sensing Cine: An Evaluation of Feasibility and Efficiency.J Clin Med. 2024 Jan 28;13(3):753. doi: 10.3390/jcm13030753. J Clin Med. 2024. PMID: 38337447 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials