

Inclusion of People Poststroke in Cardiac Rehabilitation Programs in Canada: A Missed Opportunity for Referral
- PMID: 32695969
- PMCID: PMC7365786
- DOI: 10.1016/j.cjco.2020.01.007
Inclusion of People Poststroke in Cardiac Rehabilitation Programs in Canada: A Missed Opportunity for Referral
Abstract
Background: Evidence supports establishing a continuum of care from stroke rehabilitation (SR) to cardiac rehabilitation programs (CRPs). It is not known to what extent people poststroke are being integrated. This study aimed to determine the proportion of CRPs that accept referrals poststroke, barriers/facilitators, and eligibility criteria.
Methods: A web-based questionnaire was sent to CRPs across Canada.
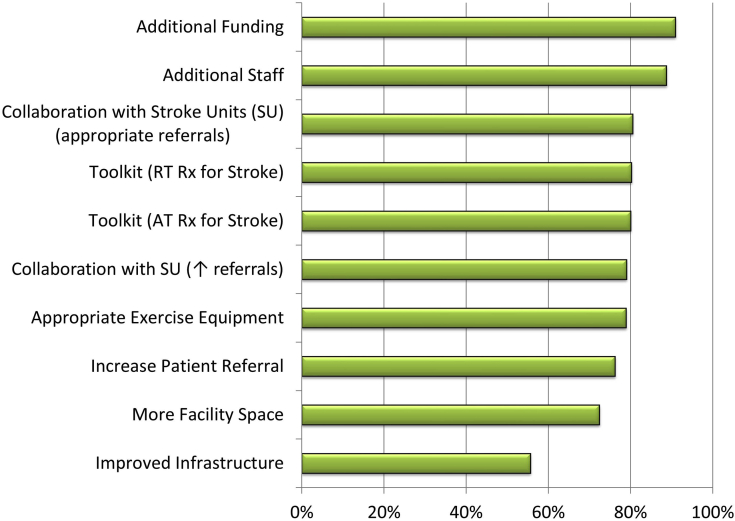
Results: Of 160 questionnaires sent, 114 representatives (71%) of 130 CRPs responded. Of respondents, 65% (n = 74) reported accepting people with a diagnosis of stroke and doing so for a median of 11 years, 11 offering stroke-specific classes and an additional 6 planning inclusion. However, 62.5% of CRPs reported that < 11 patients participated in the last calendar year despite 88.5% reporting no limit to the number they could enroll. Among CRPs, 25% accepted only patients with concurrent cardiac diagnoses, living in the community (47.8%), and without severe mobility (70.1%), communication (80.6%), or cognitive (85.1%) deficits. The 2 most influential barriers and facilitators among all CRPs were funding and staffing. The fourth greatest barrier was lack of poststroke referrals, and third to sixth facilitators were SR/CRP collaboration to ensure appropriate referrals (third) and to increase referrals (sixth), toolkits for prescribing resistance (fourth), and aerobic training (fifth). CRP characteristics associated with accepting stroke were a hybrid program model, a medium program size, and having a falls prevention component.
Conclusions: Most CRPs accept patients poststroke, but few participate. Therefore, establishing SR/CRP partnerships to increase appropriate referrals, using a toolkit to help operationalize exercise components, and allocating funding/resources to CRPs may significantly increase access to secondary prevention strategies.
Contexte: Les données recueillies appuient la continuité des soins entre les programmes de réadaptation après un accident vasculaire cérébral (PR-AVC) et les programmes de réadaptation cardiaque (PRC). On ne sait toutefois pas dans quelle mesure les patients qui ont subi un accident vasculaire cérébral (AVC) sont intégrés à un PRC. L’étude visait donc à déterminer la proportion de PRC admettant les patients ayant subi un AVC, les obstacles à l’intégration de ces derniers et les éléments qui la facilitent, ainsi que les critères d’admissibilité.
Méthodologie: Des responsables de PRC de partout au Canada ont été invités à répondre à un questionnaire en ligne.
Résultats: Au total, 160 invitations ont été envoyées et 114 (71 %) responsables rattachés à 130 PRC y ont répondu. Parmi ces répondants, 65 % (n = 74) ont dit que leur programme admettait depuis un nombre médian de 11 ans les patients ayant reçu un diagnostic d’AVC; 11 programmes offraient des cours spécialement destinés aux patients ayant subi un AVC et 6 autres prévoyaient de le faire. Toutefois, 62,5 % des répondants ont souligné que moins de 11 patients avaient participé à leur programme au cours de l’année qui précédait, malgré le fait que dans 88,5 % des cas, il n’y avait pas de limite au nombre de participants admis. Parmi les PRC, 25 % n’admettaient que des patients ayant aussi reçu un diagnostic d’atteinte cardiaque, vivant dans la collectivité (47,8 %) et n’ayant pas de déficit sévère sur les plans de la mobilité (70,1 %), de la communication (80,6 %) ou de la fonction cognitive (85,1 %). Dans tous les cas, les deux facteurs influant le plus (positivement ou négativement, selon le cas) sur l’intégration des patients ayant subi un AVC étaient les ressources financières et les ressources humaines. Le quatrième obstacle en importance était le faible nombre de patients ayant subi un AVC orientés vers les programmes; les autres éléments facilitateurs également recensés étaient la collaboration entre les PR-AVC et les PRC afin d’assurer l’orientation des patients concernés (3e place), l’augmentation du nombre de ces orientations (6e place), ainsi que les outils permettant de prescrire un programme d’entraînement musculaire (4e place) et un programme d’entraînement aérobique (5e place). Les PRC admettant des patients ayant subi un AVC avaient en commun les caractéristiques suivantes : ils reposaient sur un modèle hybride, ils étaient de taille moyenne et ils comprenaient un volet sur la prévention des chutes.
Conclusions: Si la plupart des PRC admettent les patients qui ont subi un AVC, ces derniers sont peu nombreux à y participer. L’établissement de partenariats entre les PR-AVC et les PRC afin d’augmenter le nombre de patients orientés, la mise en place d’outils facilitant l’exécution de programmes d’exercice physique et l’affectation de fonds et de ressources aux PRC pourraient donc augmenter considérablement l’accès aux stratégies de prévention secondaire.
© 2020 Canadian Cardiovascular Society. Published by Elsevier Inc.
Figures


Comment in
-
Stroke Rehabilitation and Cardiac Rehabilitation: Siblings or Strangers?CJC Open. 2020 May 23;2(4):189-191. doi: 10.1016/j.cjco.2020.05.003. eCollection 2020 Jul. CJC Open. 2020. PMID: 32697199 Free PMC article. No abstract available.
Similar articles
-
Barriers and Facilitators to Cardiovascular Rehabilitation Programmes for People with Lower Limb Amputation: A Survey of Clinical Practice in Canada.Physiother Can. 2024 May 8;76(2):199-208. doi: 10.3138/ptc-2022-0043. eCollection 2024 May. Physiother Can. 2024. PMID: 38725599 Free PMC article.
-
Inclusion of People With Peripheral Artery Disease in Cardiac Rehabilitation Programs: A Pan-Canadian Survey.Heart Lung Circ. 2021 Jul;30(7):1031-1043. doi: 10.1016/j.hlc.2020.12.018. Epub 2021 Feb 13. Heart Lung Circ. 2021. PMID: 33593677
-
Cardiac Rehabilitation in Canada During COVID-19.CJC Open. 2021 Feb;3(2):152-158. doi: 10.1016/j.cjco.2020.09.021. Epub 2020 Oct 3. CJC Open. 2021. PMID: 33521613 Free PMC article.
-
Prevalence and Related Factors for Poststroke Complex Regional Pain Syndrome: A Retrospective Cross-Sectional Cohort Study.Arch Phys Med Rehabil. 2022 Feb;103(2):274-281. doi: 10.1016/j.apmr.2021.08.003. Epub 2021 Sep 1. Arch Phys Med Rehabil. 2022. PMID: 34480888
-
Including Patients With Stroke in Cardiac Rehabilitation: BARRIERS AND FACILITATORS.J Cardiopulm Rehabil Prev. 2020 Sep;40(5):294-301. doi: 10.1097/HCR.0000000000000540. J Cardiopulm Rehabil Prev. 2020. PMID: 32868656 Review.
Cited by
-
Post pandemic research priorities: A consensus statement from the HL-PIVOT.Prog Cardiovasc Dis. 2022 Jul-Aug;73:2-16. doi: 10.1016/j.pcad.2022.07.001. Epub 2022 Jul 13. Prog Cardiovasc Dis. 2022. PMID: 35842068 Free PMC article. Review.
-
Cardiovascular Rehabilitation for transient ischaemic Attack and Mild Stroke: the CRAMS effectiveness-implementation hybrid study protocol.BMC Health Serv Res. 2022 Nov 22;22(1):1391. doi: 10.1186/s12913-022-08797-3. BMC Health Serv Res. 2022. PMID: 36419153 Free PMC article.
-
Barriers and Facilitators to Cardiovascular Rehabilitation Programmes for People with Lower Limb Amputation: A Survey of Clinical Practice in Canada.Physiother Can. 2024 May 8;76(2):199-208. doi: 10.3138/ptc-2022-0043. eCollection 2024 May. Physiother Can. 2024. PMID: 38725599 Free PMC article.
-
Mechanisms and benefits of cardiac rehabilitation in individuals with stroke: emerging role of its impact on improving cardiovascular and neurovascular health.Front Cardiovasc Med. 2024 May 2;11:1376616. doi: 10.3389/fcvm.2024.1376616. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38756753 Free PMC article. Review.
-
Stroke Rehabilitation and Cardiac Rehabilitation: Siblings or Strangers?CJC Open. 2020 May 23;2(4):189-191. doi: 10.1016/j.cjco.2020.05.003. eCollection 2020 Jul. CJC Open. 2020. PMID: 32697199 Free PMC article. No abstract available.
References
-
- Krueger H., Koot J., Hall R.E. Prevalence of individuals experiencing the effects of stroke in Canada: trends and projections. Stroke. 2015;46:2226–2231. - PubMed
-
- Hebert D., Lindsay M.P., McIntyre A. Canadian stroke best practice recommendations: stroke rehabilitation practice guidelines, update 2015. Int J Stroke. 2016;11:459–484. - PubMed
-
- Physical Activity Guidelines Advisory Committee Report. US Department of Health and Human Services. Physical Activity Guidelines Advisory Committee; Washington, DC: 2008. - PubMed
-
- Michael K.M., Macko R.F. Ambulatory activity intensity profiles, fitness, and fatigue in chronic stroke. Top Stroke Rehabil. 2007;14:5–12. - PubMed
-
- Rand D., Eng J.J., Tang P.F., Jeng J.S., Hung C. How active are people with stroke?: use of accelerometers to assess physical activity. Stroke. 2009;40:163–168. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
