

The Epidemiology of Respiratory Failure in the United States 2002-2017: A Serial Cross-Sectional Study
- PMID: 32695994
- PMCID: PMC7314331
- DOI: 10.1097/CCE.0000000000000128
The Epidemiology of Respiratory Failure in the United States 2002-2017: A Serial Cross-Sectional Study
Abstract
Objectives: Respiratory failure with mechanical ventilation is a limited labor-intensive resource that is associated with high mortality. Understanding the longitudinal national epidemiology is essential for the organization of healthcare resources.
Design: Serial cross-sectional study.
Setting: The 2002-2017 Healthcare Utilization Project's National Inpatient Sample datasets.
Interventions: None.
Measurements: We use six diagnosis codes and five procedural codes from International Classification of Diseases, 9th Revision, Clinical Modification, and 19 diagnosis codes and 15 procedures codes from International Classification of Diseases, 10th Revision, Clinical Modification to examine national epidemiology of different case definitions for respiratory failure.
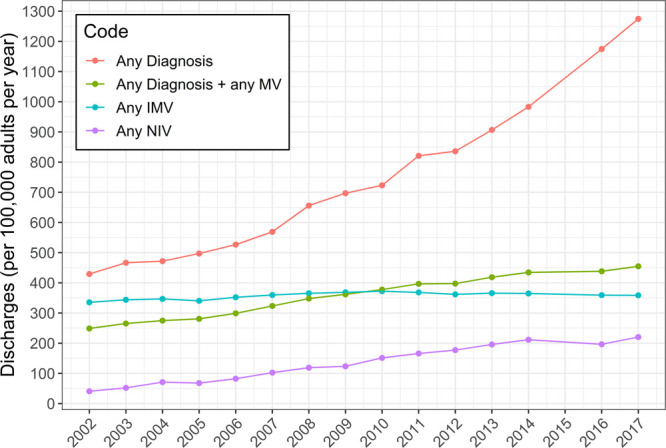
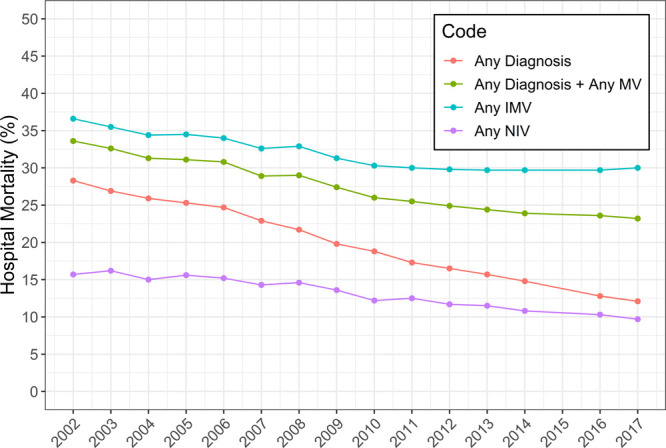
Results: In the United States in 2017, there were an estimated 1,146,195 discharges with a diagnosis of respiratory failure and procedural code for mechanical ventilation, with an average length of stay of 10.5 days and hospital charge of $158,443. Over the study period, there was an 83% increase in incidence from 249 to 455 cases per 100,000 adults with a 48% decrease in hospital mortality from 34% to 23%. Exploring a case definition that captures only diagnosis codes for respiratory failure, there was a 197% increase in annual incidence, from 429 to 1,275 cases per 100,000 adults with a 57% decrease in hospital mortality from 28% to 12%. For invasive mechanical ventilation without a requisite diagnosis code, there was no change in incidence over the study period, with the 2017 incidence at 359 cases per 100,000 adults, but a 19% decrease in hospital mortality from 37% to 30%. For the noninvasive mechanical ventilation procedural codes, there was a 437% increase in incidence from 41 to 220 cases per 100,000 adults, with a 38% decrease in hospital mortality from 16% to 10%.
Conclusions: Examining different case definitions for respiratory failure, there was a large increase in the population incidence and decrease in the hospital mortality for respiratory failure diagnosis codes with more modest changes procedural codes for invasive mechanical ventilation. There was a large increase in incidence of noninvasive mechanical ventilation.
Keywords: epidemiology; health services research; mechanical ventilation; respiratory failure.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Kempker received support from the Agency for Healthcare Quality and Research (K08HS025240) and has received consulting fees from Grifols. Dr. Martin received research support from the National Institutes of Health’s National Center for Advancing Translational Science (UL1 TR-002378) and the Marcus Foundation and has served as a consultant for Grifols. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
