

VO2max-Based Physical Fitness Categories in a Brazilian Population with Supposed High Socioeconomic Status and without Structural Heart Disease
- PMID: 32696857
- PMCID: PMC9363094
- DOI: 10.36660/abc.20190189
VO2max-Based Physical Fitness Categories in a Brazilian Population with Supposed High Socioeconomic Status and without Structural Heart Disease
Abstract
Background: The most widely used data for cardiorespiratory fitness (CRF) referrals are from the Cooper Clinic, which uses calculated maximal oxygen uptake (VO2max) values.
Objective: To develop CRF values from cardiopulmonary exercise testing (CPX) in a Brazilian population with high socioeconomic level and free of structural heart disease. VO2max testing results were compared with the Cooper Clinic and FRIEND Registry data.
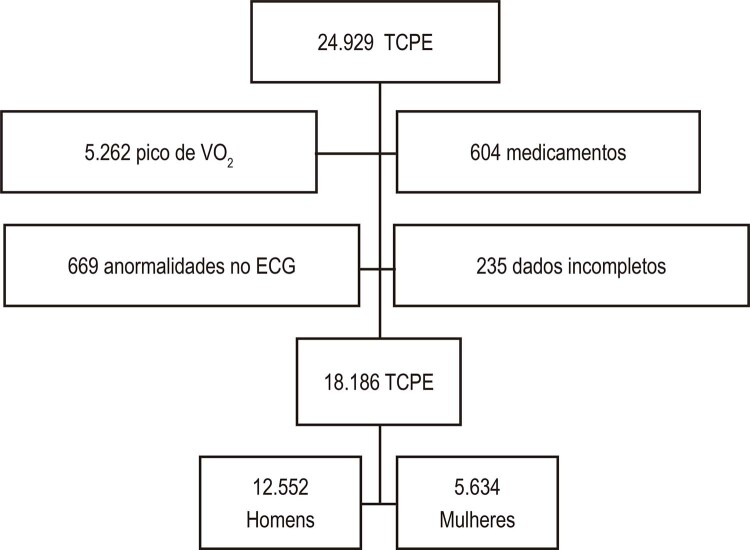
Methods: CPX data from consecutive individuals between January 1,2000, and May 31,2016 were used in this study. Inclusion criteria were: VO2max by a pre-specified definition. We built a CRF chart according to VO2max percentiles: very poor (≤20%), poor (20-40%), fair (40-60%), good (60-80%), excellent (80-90%), and superior (≥90%). Kappa correlation was used to analyze our data in comparison with that of the other two databases. Statistical tests with p<0.005 were considered significant.
Results: Final cohort included 18,186 tests: 12,552 men, 5,634 women (7-84 years). The most recurrent response was "good" (20.2%). There was a mean difference in weight, height, body mass index (BMI), and age in the CRF chart. An inverse correlation existed between VO2max and age, weight, and BMI. Using a linear regression and these variables, a predictive equation was developed for VO2max. Our findings differed from that of the other databases.
Conclusion: We developed a classification for CRF and found higher values in all classification ranges of functional capacity in contrast to the Cooper Clinic and FRIEND Registry. Our findings offer a more accurate interpretation of ACR in this large Brazilian population sample when compared to previous standards based on the estimated VO2max. (Arq Bras Cardiol. 2020; 115(3):468-477).
Fundamento: Os dados mais utilizados como referência de aptidão cardiorrespiratória (ACR) são os de Cooper, que utiliza valores calculados de captação máxima de oxigênio (VO2máx).
Objetivo: Desenvolver valores de ACR a partir do teste cardiopulmonar de exercício (TCPE) em uma população brasileira com alto nível socioeconômico e livre de cardiopatia estrutural. Os resultados dos testes de VO2max foram comparados aos dados de Cooper e do FRIEND Registry.
Métodos: Foram utilizados neste estudo dados de TCPE de indivíduos consecutivos entre 1º de janeiro de 2000 e 31 de maio de 2016. Os critérios de inclusão foram: VO2máx pré-definido. Foi construído um gráfico de ACR de acordo com os percentuais do VO2máx: muito ruim (≤20%), ruim (20-40%), regular (40-60%), boa (60-80%), excelente (80-90%), e superior (≥90%). A correlação Kappa foi usada para analisar nossos dados em comparação aos dados dos outros dois bancos de dados. Os testes estatísticos com p<0,005 foram considerados significativos.
Resultados: A coorte final incluiu 18.186 testes: 12.552 homens, 5.634 mulheres (7 a 84 anos). A resposta mais recorrente foi “boa” (20,2%). Houve diferença média de peso, altura, índice de massa corporal (IMC) e idade no gráfico da ACR. Houve correlação inversa entre VO2máx e idade, peso e IMC. Usando uma regressão linear e essas variáveis, uma equação preditiva foi desenvolvida para o VO2máx. Nossas descobertas diferiram das dos outros bancos de dados.
Conclusão: Desenvolvemos uma classificação para a ACR e encontramos valores mais altos em todas as faixas de classificação de capacidade funcional, em contraste com os dados de Cooper e do FRIEND Registry. Nossos achados oferecem uma interpretação mais precisa da ACR nessa grande amostra populacional brasileira, quando comparados aos padrões anteriores, com base no VO2máx estimado. (Arq Bras Cardiol. 2020; 115(3):468-477).
Conflict of interest statement
Potencial conflito de interesses
Declaro não haver conflito de interesses pertinentes.
Figures

Comment in
-
Oxygen Consumption and Cardiorespiratory Fitness. The Difference between Chronological and Biological Age.Arq Bras Cardiol. 2020 Sep;115(3):478-479. doi: 10.36660/abc.20200582. Arq Bras Cardiol. 2020. PMID: 33027369 Free PMC article. English, Portuguese. No abstract available.
Similar articles
-
Reference Standards for Cardiorespiratory Fitness Measured With Cardiopulmonary Exercise Testing Using Cycle Ergometry: Data From the Fitness Registry and the Importance of Exercise National Database (FRIEND) Registry.Mayo Clin Proc. 2017 Feb;92(2):228-233. doi: 10.1016/j.mayocp.2016.10.003. Epub 2016 Dec 7. Mayo Clin Proc. 2017. PMID: 27938891
-
Cardiorespiratory fitness data from 18,189 participants who underwent treadmill cardiopulmonary exercise testing in a Brazilian population.PLoS One. 2019 Jan 9;14(1):e0209897. doi: 10.1371/journal.pone.0209897. eCollection 2019. PLoS One. 2019. PMID: 30625200 Free PMC article.
-
A reference equation for maximal aerobic power for treadmill and cycle ergometer exercise testing: Analysis from the FRIEND registry.Eur J Prev Cardiol. 2018 May;25(7):742-750. doi: 10.1177/2047487318763958. Epub 2018 Mar 8. Eur J Prev Cardiol. 2018. PMID: 29517365
-
Cardiorespiratory fitness in breast cancer patients: a call for normative values.J Am Heart Assoc. 2014 Jan 13;3(1):e000432. doi: 10.1161/JAHA.113.000432. J Am Heart Assoc. 2014. PMID: 24419734 Free PMC article. Review.
-
Temporal trends in the cardiorespiratory fitness of children and adolescents representing 19 high-income and upper middle-income countries between 1981 and 2014.Br J Sports Med. 2019 Apr;53(8):478-486. doi: 10.1136/bjsports-2017-097982. Epub 2017 Oct 30. Br J Sports Med. 2019. PMID: 29084727
Cited by
-
Brazilian Guideline for Exercise Test in the Adult Population - 2024.Arq Bras Cardiol. 2024 Feb;121(3):e20240110. doi: 10.36660/abc.20240110. Arq Bras Cardiol. 2024. PMID: 38896581 Free PMC article. English, Portuguese. No abstract available.
-
Oxygen Consumption and Cardiorespiratory Fitness. The Difference between Chronological and Biological Age.Arq Bras Cardiol. 2020 Sep;115(3):478-479. doi: 10.36660/abc.20200582. Arq Bras Cardiol. 2020. PMID: 33027369 Free PMC article. English, Portuguese. No abstract available.
References
-
- 1. Ross R, Blair SN, Arena R, Church TS, Després J-P, Franklin BA, et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement From the American Heart Association. Circulation. 2016 13;134(24):e653–99. - PubMed
-
- 2. Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301(19):2024–35. - PubMed
-
- 3. Kokkinos P, Myers J. Exercise and physical activity: clinical outcomes and applications. Circulation. 2010;122(16):1637–48. - PubMed
-
- 4. Wicks JR, Oldridge NB. How Accurate Is the Prediction of Maximal Oxygen Uptake with Treadmill Testing? PLoS One [Internet]. 2016 Nov 22 [cited 2019 Mar 6];11(11). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5119771/ - PMC - PubMed
-
- 5. Farrell SW, Finley CE, Radford NB, Haskell WL. Cardiorespiratory fitness, body mass index, and heart failure mortality in men: Cooper Center Longitudinal Study. Circ Heart Fail. 2013;6(5):898–905. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
