

Adult ICU Triage During the Coronavirus Disease 2019 Pandemic: Who Will Live and Who Will Die? Recommendations to Improve Survival
- PMID: 32697491
- PMCID: PMC7217126
- DOI: 10.1097/CCM.0000000000004410
Adult ICU Triage During the Coronavirus Disease 2019 Pandemic: Who Will Live and Who Will Die? Recommendations to Improve Survival
Abstract
Objectives: Coronavirus disease 2019 patients are currently overwhelming the world's healthcare systems. This article provides practical guidance to front-line physicians forced to make critical rationing decisions.
Data sources: PubMed and Medline search for scientific literature, reviews, and guidance documents related to epidemic ICU triage including from professional bodies.
Study selection: Clinical studies, reviews, and guidelines were selected and reviewed by all authors and discussed by internet conference and email.
Data extraction: References and data were based on relevance and author consensus.
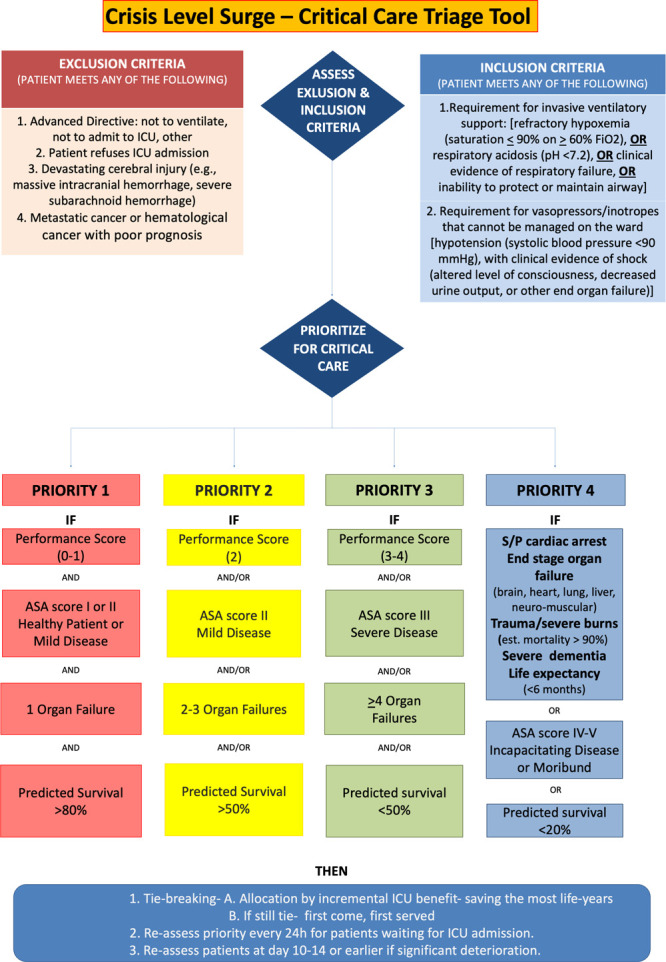
Data synthesis: We review key challenges of resource-driven triage and data from affected ICUs. We recommend that once available resources are maximally extended, triage is justified utilizing a strategy that provides the greatest good for the greatest number of patients. A triage algorithm based on clinical estimations of the incremental survival benefit (saving the most life-years) provided by ICU care is proposed. "First come, first served" is used to choose between individuals with equal priorities and benefits. The algorithm provides practical guidance, is easy to follow, rapidly implementable and flexible. It has four prioritization categories: performance score, ASA score, number of organ failures, and predicted survival. Individual units can readily adapt the algorithm to meet local requirements for the evolving pandemic. Although the algorithm improves consistency and provides practical and psychologic support to those performing triage, the final decision remains a clinical one. Depending on country and operational circumstances, triage decisions may be made by a triage team or individual doctors. However, an experienced critical care specialist physician should be ultimately responsible for the triage decision. Cautious discharge criteria are proposed acknowledging the difficulties to facilitate the admission of queuing patients.
Conclusions: Individual institutions may use this guidance to develop prospective protocols that assist the implementation of triage decisions to ensure fairness, enhance consistency, and decrease provider moral distress.
Figures
Comment in
-
Coronavirus Disease 2019 Triage Teams: Death by Numbers.Crit Care Med. 2020 Aug;48(8):1241-1242. doi: 10.1097/CCM.0000000000004435. Crit Care Med. 2020. PMID: 32697500 Free PMC article. No abstract available.
-
Saving Lives Versus Saving Dollars: The Acceptable Loss for Coronavirus Disease 2019.Crit Care Med. 2020 Aug;48(8):1243-1244. doi: 10.1097/CCM.0000000000004452. Crit Care Med. 2020. PMID: 32697501 Free PMC article. No abstract available.
-
The Triage Stalemate During the Coronavirus Disease 2019 Pandemic: Losing Fairness to Ethical Paralysis.Crit Care Med. 2020 Dec;48(12):e1380-e1381. doi: 10.1097/CCM.0000000000004567. Crit Care Med. 2020. PMID: 32826433 Free PMC article. No abstract available.
References
-
- Simchen E, Sprung CL, Galai N, et al. Survival of critically ill patients hospitalized in and out of intensive care units under paucity of intensive care unit beds. Crit Care Med 2004; 32:1654–1661 - PubMed
-
- Sprung CL, Artigas A, Kesecioglu J, et al. The Eldicus prospective, observational study of triage decision making in European intensive care units. Part II: Intensive care benefit for the elderly. Crit Care Med 2012; 40:132–138 - PubMed
-
- Wunsch H, Angus DC, Harrison DA, et al. Variation in critical care services across North America and Western Europe. Crit Care Med 2008; 36:2787–2793, e1–e9 - PubMed
-
- Rosenbaum L. Facing Covid-19 in Italy - ethics, logistics, and therapeutics on the epidemic’s front line. N Engl J Med. 2020 Mar 18. [online ahead of print] - PubMed
-
- Consensus statement on the triage of critically ill patients. Society of Critical Care Medicine. Ethics Committee. JAMA 1994; 271:1200–1203 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
