

Current State of Knowledge on Primary Sjögren's Syndrome, an Autoimmune Exocrinopathy
- PMID: 32698400
- PMCID: PMC7408693
- DOI: 10.3390/jcm9072299
Current State of Knowledge on Primary Sjögren's Syndrome, an Autoimmune Exocrinopathy
Abstract
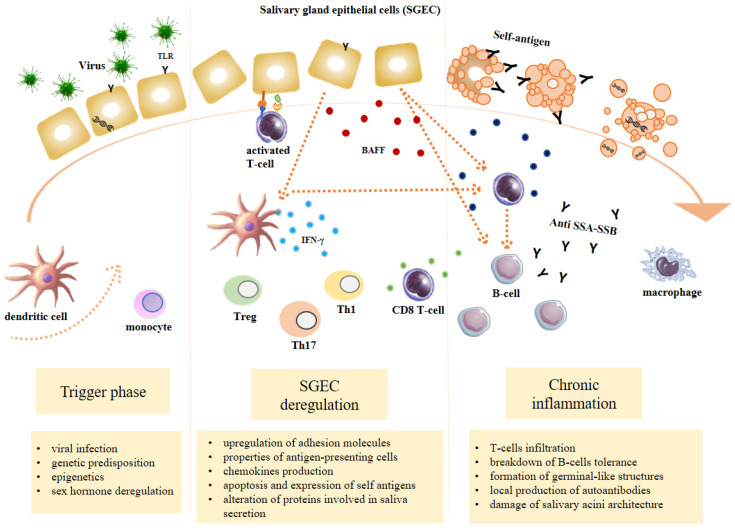
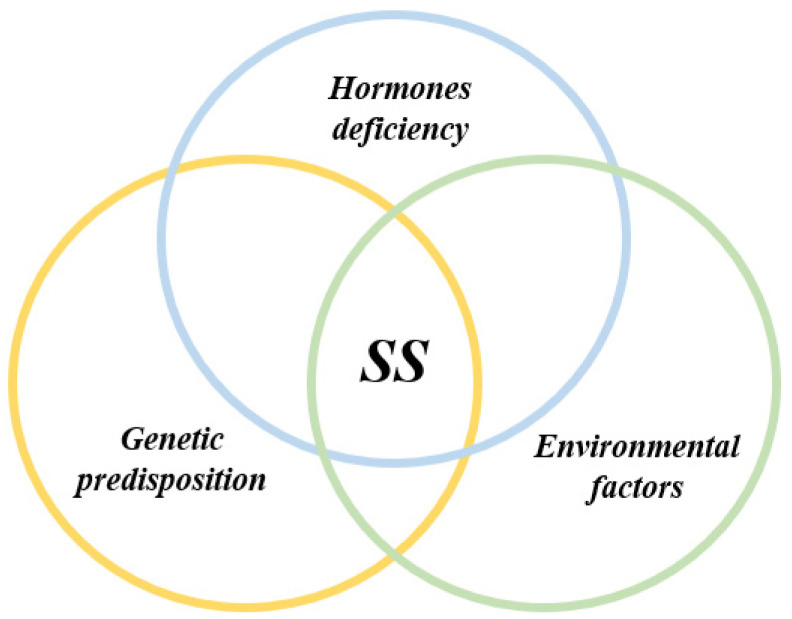
Primary Sjögren's syndrome (pSS) is a chronic systemic autoimmune rheumatic disease characterized by lymphoplasmacytic infiltration of the salivary and lacrimal glands, whereby sicca syndrome and/or systemic manifestations are the clinical hallmarks, associated with a particular autoantibody profile. pSS is the most frequent connective tissue disease after rheumatoid arthritis, affecting 0.3-3% of the population. Women are more prone to develop pSS than men, with a sex ratio of 9:1. Considered in the past as innocent collateral passive victims of autoimmunity, the epithelial cells of the salivary glands are now known to play an active role in the pathogenesis of the disease. The aetiology of the "autoimmune epithelitis" still remains unknown, but certainly involves genetic, environmental and hormonal factors. Later during the disease evolution, the subsequent chronic activation of B cells can lead to the development of systemic manifestations or non-Hodgkin's lymphoma. The aim of the present comprehensive review is to provide the current state of knowledge on pSS. The review addresses the clinical manifestations and complications of the disease, the diagnostic workup, the pathogenic mechanisms and the therapeutic approaches.
Keywords: Sjögren’s syndrome; autoimmune disease; diagnosis; physiopathology; review; treatment.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Gerli R., Bartoloni E., Alunno A., editors. Sjögren’s Syndrome: Novel Insights in Pathogenic, Clinical, and Therapeutic Aspects. Elsevier; Amsterdam, The Netherlands: Academic Press; Cambridge, MA, USA: 2016.
-
- Wollheim F.A. Henrik Sjögren and Sjögren’s syndrome. Scand. J. Rheumatol. Suppl. 1986;61:11–16. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
