

Outcome of bilateral hip reconstruction in unilateral hip subluxation in cerebral palsy: Comparison to unilateral hip reconstruction
- PMID: 32699490
- PMCID: PMC7363623
- DOI: 10.1016/j.jor.2020.06.017
Outcome of bilateral hip reconstruction in unilateral hip subluxation in cerebral palsy: Comparison to unilateral hip reconstruction
Erratum in
-
Erratum regarding missing Declaration of Competing Interest statements in previously published articles.J Orthop. 2020 Dec 15;24:291. doi: 10.1016/j.jor.2020.12.004. eCollection 2021 Mar-Apr. J Orthop. 2020. PMID: 33994700 Free PMC article.
Abstract
Objective: To evaluate the post-operative outcomes of the hips in CP patients with unilateral hip subluxation treated with bilateral and unilateral hip reconstruction.
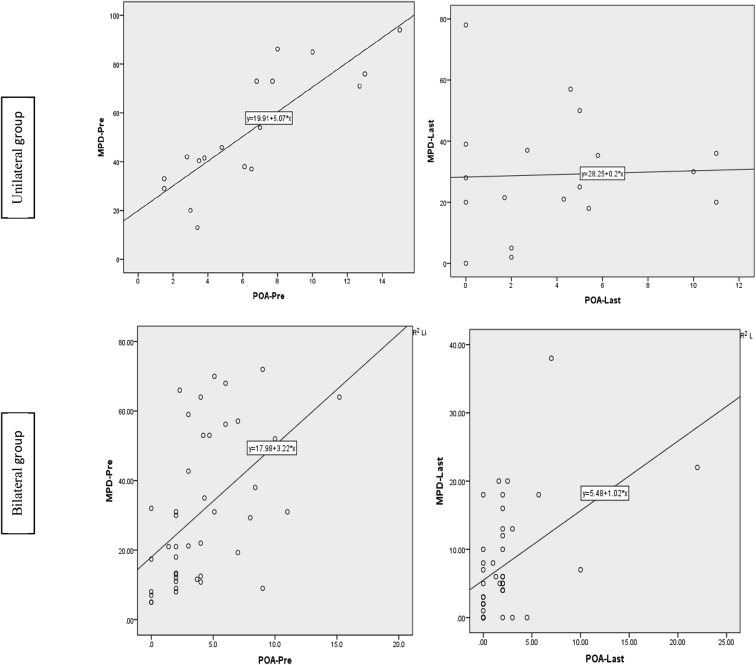
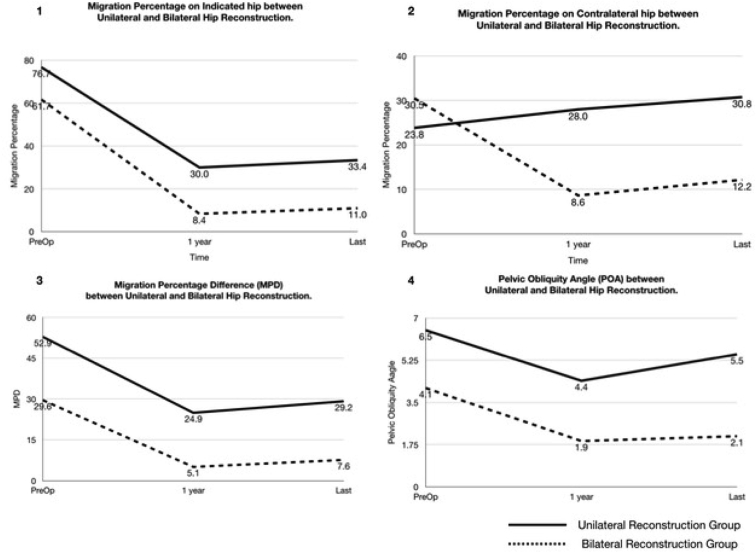
Methods: A retrospective review was performed of all diplegic and quadriplegic patients with unilateral hip displacement treated with either bilateral or unilateral hip reconstructive surgery. Radiographic parameters [migration percentage (MP), pelvic obliquity angle (POA) and migration percentage difference (MPD)] and changes in functional ability (sitting, standing and walking) were evaluated and compared between the 2 groups. Failure was defined as post-operative MP>40%, POA>5° and MPD>30%.
Results: Eighteen patients had unilateral hip reconstruction and 42 patients had bilateral hip reconstruction. Mean age of 87 months and 90 months and means follow-up of 38 months and 40 months respectively. Post-operative MP was significant in both groups. However, of 18 patients in unilateral hip reconstruction group, 33.3% of patients had contralateral hip subluxation and 22.2% of patients had hip failure on the operated hip; compared to only one of 42 patients had hip failure and no contralateral hip problem in the other group. For assessment of pelvic symmetry, MPD was significantly improved in both group but POA was only significant in bilateral group. Overall functional improvement was significant in patients with bilateral hip reconstruction compared to unilateral group.
Conclusion: Bilateral hip reconstruction in unilateral displacement had shown to have better outcome in correcting unstable hip and pelvic asymmetry, thus provide good sitting balance and improvement in overall functional outcome.
Keywords: Bilateral hip reconstruction; Cerebral palsy; Functional outcome; Pelvic obliquity; Prophylactic hip reconstruction; Unilateral/contralateral hip subluxation.
© 2020 Professor P K Surendran Memorial Education Foundation. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Terjesen T. The natural history of hip development in cerebral palsy. Dev Med Child Neurol. 2012;54(10):951–957. - PubMed
-
- Pruszczynski B., Sees J., Miller F. Risk factors for hip displacement in children with cerebral palsy: systematic review. J Pediatr Orthop. 2016;36(8):829–833. - PubMed
-
- Flynn J.M., Miller F. Management of hip disorders in patients with cerebral palsy. J Am Acad Orthop Surg. 2002;10:198–209. - PubMed
-
- Moreau M., Drummond D.S., Rogala E. Natural history of the dislocated hip in spastic cerebral palsy. Dev Med Child Neurol. 1979;21:749–753. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
