

Kidney disease and electrolytes in COVID-19: more than meets the eye
- PMID: 32699613
- PMCID: PMC7367104
- DOI: 10.1093/ckj/sfaa112
Kidney disease and electrolytes in COVID-19: more than meets the eye
Abstract
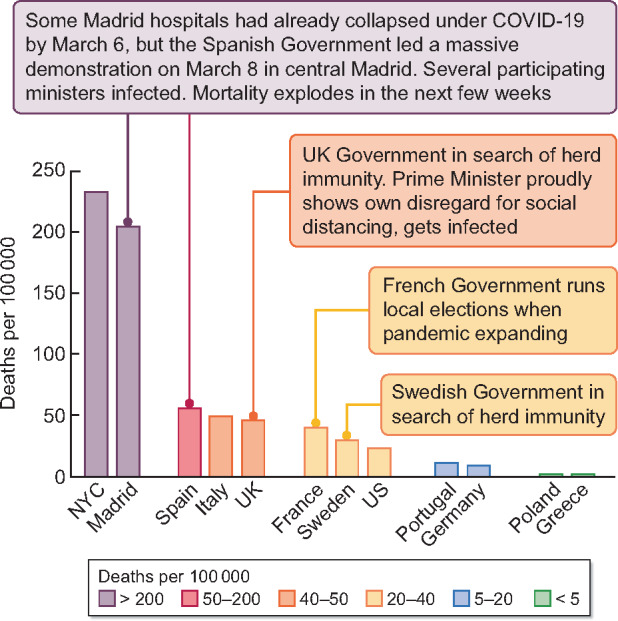
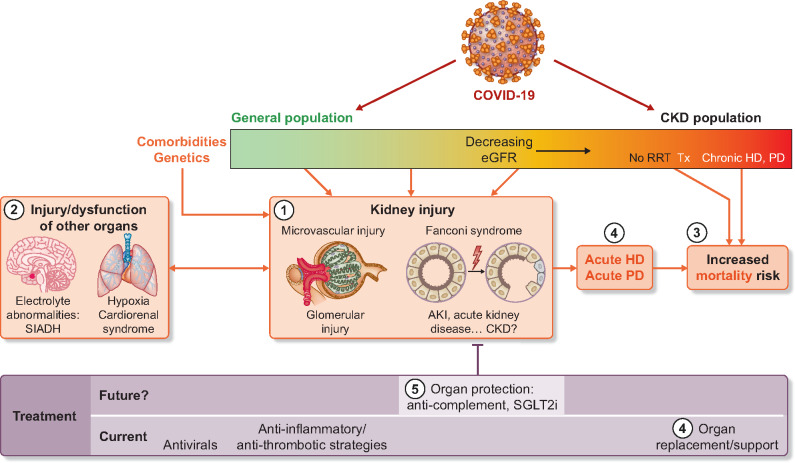
COVID-19 is a global pandemic fuelled in some countries by government actions. The current issue of Clinical Kidney Journal presents 15 articles on COVID-19 and kidney disease from three continents, providing a global perspective of the impact of severe acute respiratory syndrome coronavirus 2 on electrolytes and different kidney compartments (glomeruli, tubules and vascular compartments) and presenting clinically as a syndrome of inappropriate antidiuretic hormone secretion, acute kidney injury, acute kidney disease, collapsing glomerulopathy and thrombotic microangiopathy, among others, in the context of a brand-new cardiorenal syndrome. Kidney injury may need acute dialysis that may overwhelm haemodialysis (HD) and haemofiltration capabilities. In this regard, acute peritoneal dialysis (PD) may be lifesaving. Additionally, pre-existent chronic kidney disease increases the risk of more severe COVID-19 complications. The impact of COVID-19 on PD and HD patients is also discussed, with emphasis on preventive measures. Finally, current therapeutic approaches and potential future therapeutic approaches undergoing clinical trials, such as complement targeting by eculizumab, are also presented.
Keywords: APOL1; COVID-19; Fanconi; SIADH; acute kidney injury; cardiorenal; chronic kidney disease; haemodialysis; peritoneal dialysis.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA.
Figures

References
-
- World Health Organization. WHO Timeline - COVID-19. https://www.who.int/news-room/detail/27-04-2020-who-timeline—-covid-19 (...
-
- European Centres for Disease Prevention and Control. ECDC assessment of the COVID-19 situation in Europe as of 2 March 2020. https://www.ecdc.europa.eu/en/news-events/ecdc-assessment-covid-19-situa... (9 May 2020, date last accessed)
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
