

Bridging-to-Surgery in Patients with Type 2 Intestinal Failure
- PMID: 32700102
- PMCID: PMC8203517
- DOI: 10.1007/s11605-020-04741-0
Bridging-to-Surgery in Patients with Type 2 Intestinal Failure
Abstract
Aim: Type 2 intestinal failure (IF) is characterized by the need for longer-term parenteral nutrition (PN). During this so-called bridging-to-surgery period, morbidity and mortality rates are high. This study aimed to evaluate to what extent a multidisciplinary IF team is capable to safely guide patients towards reconstructive surgery.
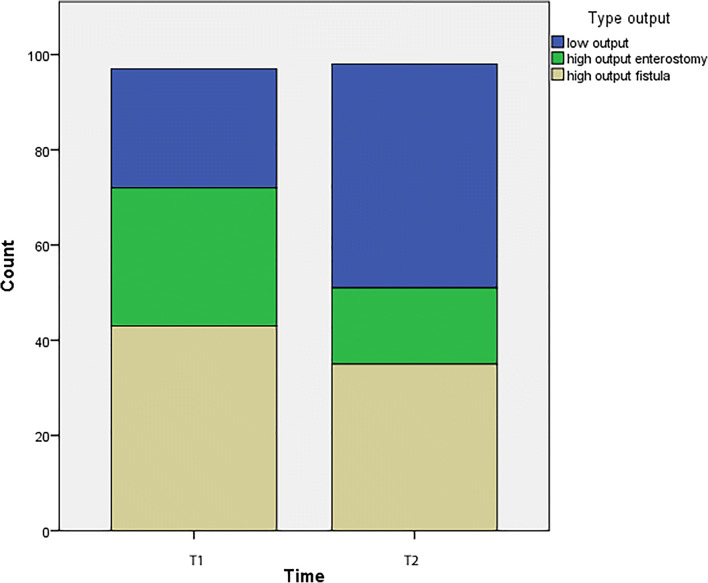
Methods: A consecutive series of patients with type 2 IF followed up by a specialized IF team between January 1st, 2011, and March 1st, 2016, was analyzed. Data on their first outpatient clinic visit (T1) and their last visit before reconstructive surgery (T2) was collected. The primary outcome was a combined endpoint of a patient being able to recover at home, have (partial) oral intake, and a normal albumin level (> 35 g/L) before surgery.
Results: Ninety-three patients were included. The median number of previous abdominal procedures was 4. At T2 (last visit prior to reconstructive surgery), significantly more patients met the combined primary endpoint compared with T1 (first IF team consultation) (66.7% vs. 28.0% (p < 0.0001), respectively); 86% had home PN. During "bridging-to-surgery," acute hospitalization rate was 40.9% and acute surgery was 4.3%. Postoperatively, 44.1% experienced a major complication, 5.4% had a fistula, and in-hospital mortality was 6.5%. Of the cohort, 86% regained enteral autonomy, and when excluding in-hospital mortality and incomplete follow-up, this was 94.1%. An albumin level < 35 g/L at T2 and weight loss of > 10% at T2 compared with preadmission weight were significant risk factors for major complications.
Conclusion: Bridging-to-surgery of type 2 IF patients under the guidance of an IF team resulted in the majority of patients being managed at home, having oral intake, and restored albumin levels prior to reconstructive surgery compared with their first IF consultation.
Keywords: Intestinal failure type 2; bridging-to-surgery; fistula; high-output; parenteral nutrition; stoma.
Conflict of interest statement
M.A. Boermeester reports institutional grants from Baxter BV, Acelity, LifeCell, and Ipsen, during the conduct of the study, and grants from Johnson&Johnson, Bard Mylan, outside the submitted work.
M.J. Serlie reports institutional grants from Baxter BV and TEFA Mediq BV during the conduct of the study. The other authors declare no conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
