

Use of age-dependent FRAX-based intervention thresholds for Singapore
- PMID: 32700118
- PMCID: PMC7376084
- DOI: 10.1007/s11657-020-00782-9
Use of age-dependent FRAX-based intervention thresholds for Singapore
Abstract
Assessment and treatment pathways based on age-specific intervention thresholds in Singapore using FRAX paths can be used to identify patients at high risk of fracture and avoid unnecessary treatment in those at low risk.
Purpose: Intervention thresholds for the treatment of osteoporosis have been based historically on the measurement of bone mineral density. The development of FRAX® has permitted a more accurate assessment of fracture risk. The aim of the present study was to explore treatment paths and characteristics of women selected for treatment in Singapore based on FRAX.
Methods: The approach to the setting of intervention and assessment thresholds used the methodology adopted by the National Osteoporosis Guideline Group for FRAX-based guidelines in the UK but based on the epidemiology of fracture and death in Singapore. The methodology was applied to women age 50 years or more drawn from the population-based Singapore Chinese Health Study (SCHS) cohort. Missing data for the calculation of FRAX was simulated using data from Chinese cohorts from Hong Kong.
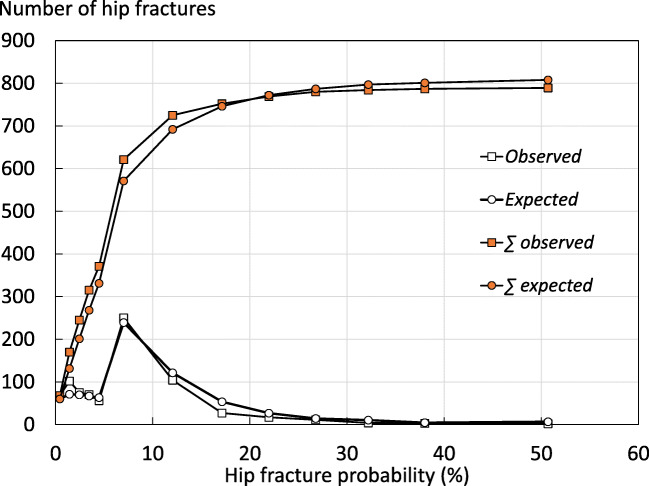
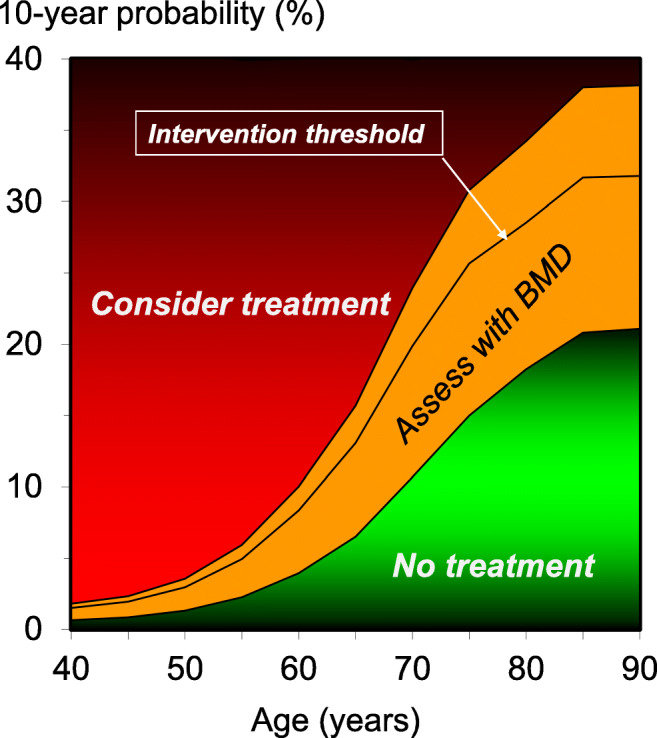
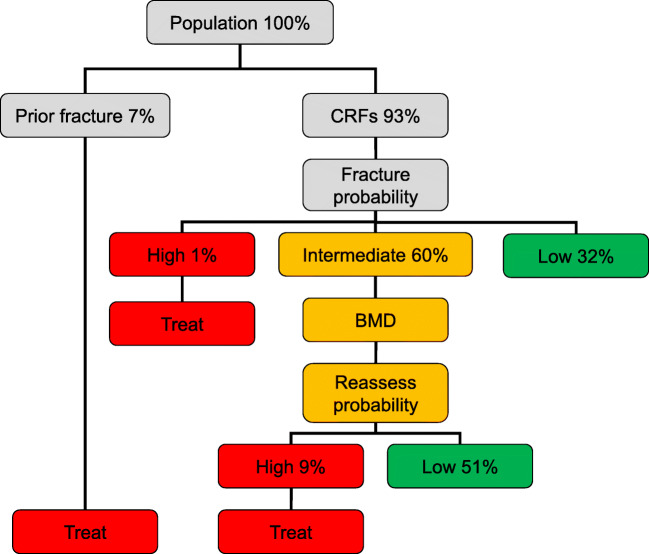
Results: Intervention thresholds expressed as a 10-year probability of a major osteoporotic fracture ranged from 2.9% at the age of 50 years increasing to 32% at the age of 90 years. A total of 1927 of 29,323 women (7%) had a prior fragility fracture and would be eligible for treatment for this reason. An additional 3019 women (10.3%) would be eligible for treatment on the basis of age-dependent thresholds. The mean BMD T-score of women so selected was -2.94.
Conclusion: Probability-based assessment of fracture risk using age-specific intervention thresholds was developed for Singapore to help guide decisions about treatment.
Keywords: FRAX; Fracture risk assessment; Intervention threshold; Osteoporosis.
Conflict of interest statement
John A Kanis, Manju Chandran, Siok Bee Chionh, Ganga Ganeson, Nicholas C Harvey, Woon-Puay Koh, Timothy Kwok, Tang Ching Lau, Enwu Liu, Mattias Lorentzon, Eugene V McCloskey, Kelvin Bryan Tan, Liesbeth Vandenput, and Helena Johansson declare no conflicts of interest in relation to this paper. JAK, NH, ML, EVM, HJ, ML, LV, and EL are responsible for the creation and/or maintenance of FRAX but have no financial interest.
Figures
References
-
- Chandran M, Lau TC, Gagnon-Arpin I, Dobrescu A, Li W, Leung MYM, Patil N, Zhao Z. The health and economic burden of osteoporotic fractures in Singapore and the potential impact of increasing treatment rates through more pharmacological options. Arch Osteoporos. 2019;14:114. doi: 10.1007/s11657-019-0664-4. - DOI - PubMed
-
- Hernlund E, Svedbom A, Ivergård M, Compston J, Cooper C, Stenmark J, McCloskey EV, Jönsson B, Kanis JA. Osteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA) Arch Osteoporos. 2013;8:136. doi: 10.1007/s11657-013-0136-1. - DOI - PMC - PubMed
-
- Kanis JA, Cooper C, Rizzoli R, Reginster J-Y, Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis (ESCEO) and the Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation (IOF) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2019;30:3–44. doi: 10.1007/s00198-018-4704-5. - DOI - PMC - PubMed
-
- Kanis JA On behalf of the World Health Organization scientific group (2008) assessment of osteoporosis at the primary healthcare level. Technical report. WHO collaborating Centre, University of Sheffield, UK. Available at . http://www.shef.ac.uk/FRAX/pdfs/WHO_Technical_Report.pdf. Accessed 26 Feb 2019
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
