

National Trends in Potentially Preventable Hospitalizations of Older Adults with Dementia
- PMID: 32700399
- PMCID: PMC7811187
- DOI: 10.1111/jgs.16636
National Trends in Potentially Preventable Hospitalizations of Older Adults with Dementia
Abstract
Background/objectives: Dementia is associated with higher healthcare expenditures, in large part due to increased hospitalization rates relative to patients without dementia. Data on contemporary trends in the incidence and outcomes of potentially preventable hospitalizations of patients with dementia are lacking.
Design: Retrospective cohort study using the National Inpatient Sample from 2012 to 2016.
Setting: U.S. acute care hospitals.
Participants: A total of 1,843,632 unique hospitalizations of older adults (aged ≥65 years) with diagnosed dementia.
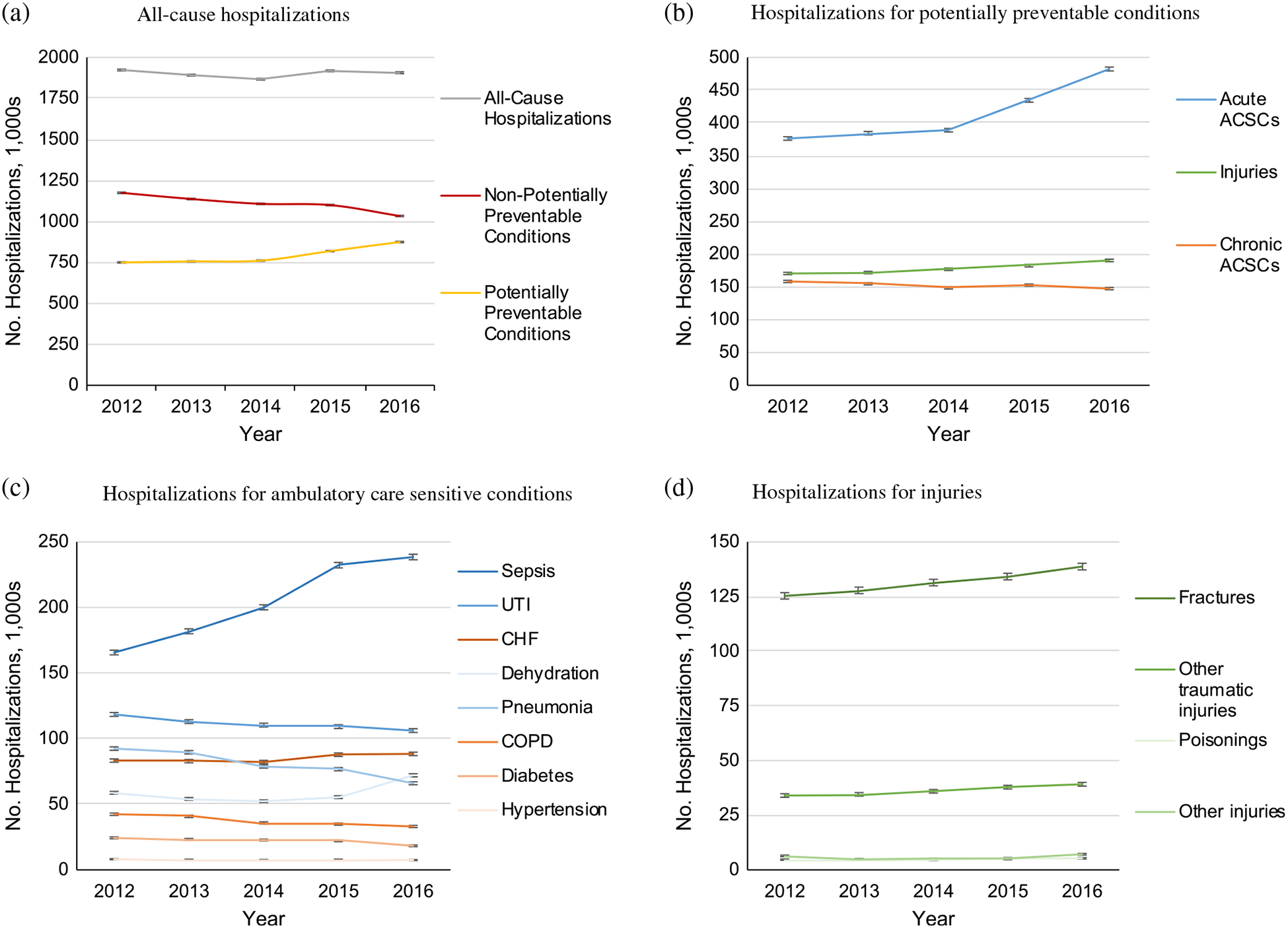
Measurements: Annual trends in the incidence of hospitalizations for all causes and for potentially preventable conditions including acute ambulatory care sensitive conditions (ACSCs), chronic ACSCs, and injuries. In-hospital outcomes including mortality, discharge disposition, and hospital costs.
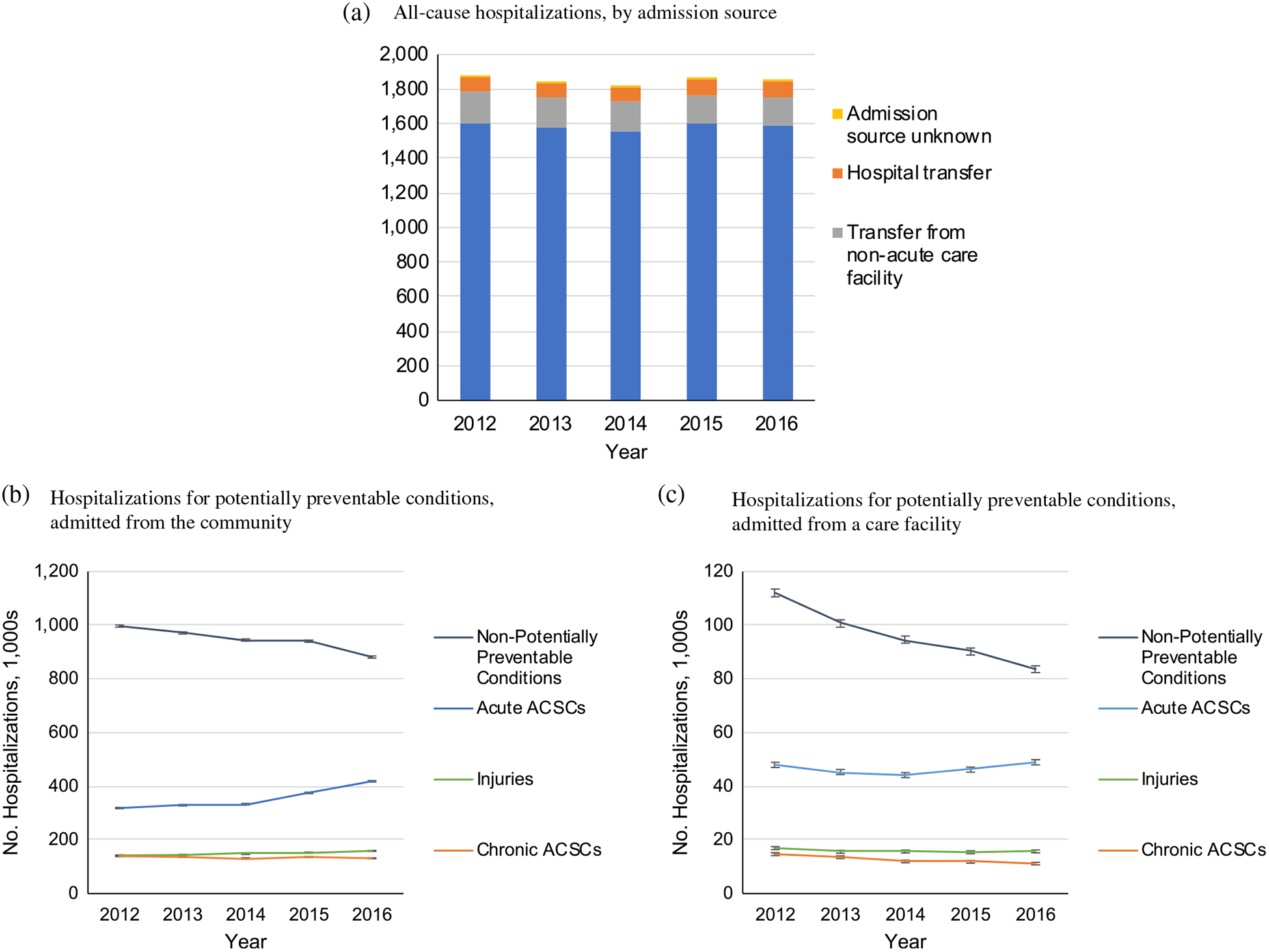
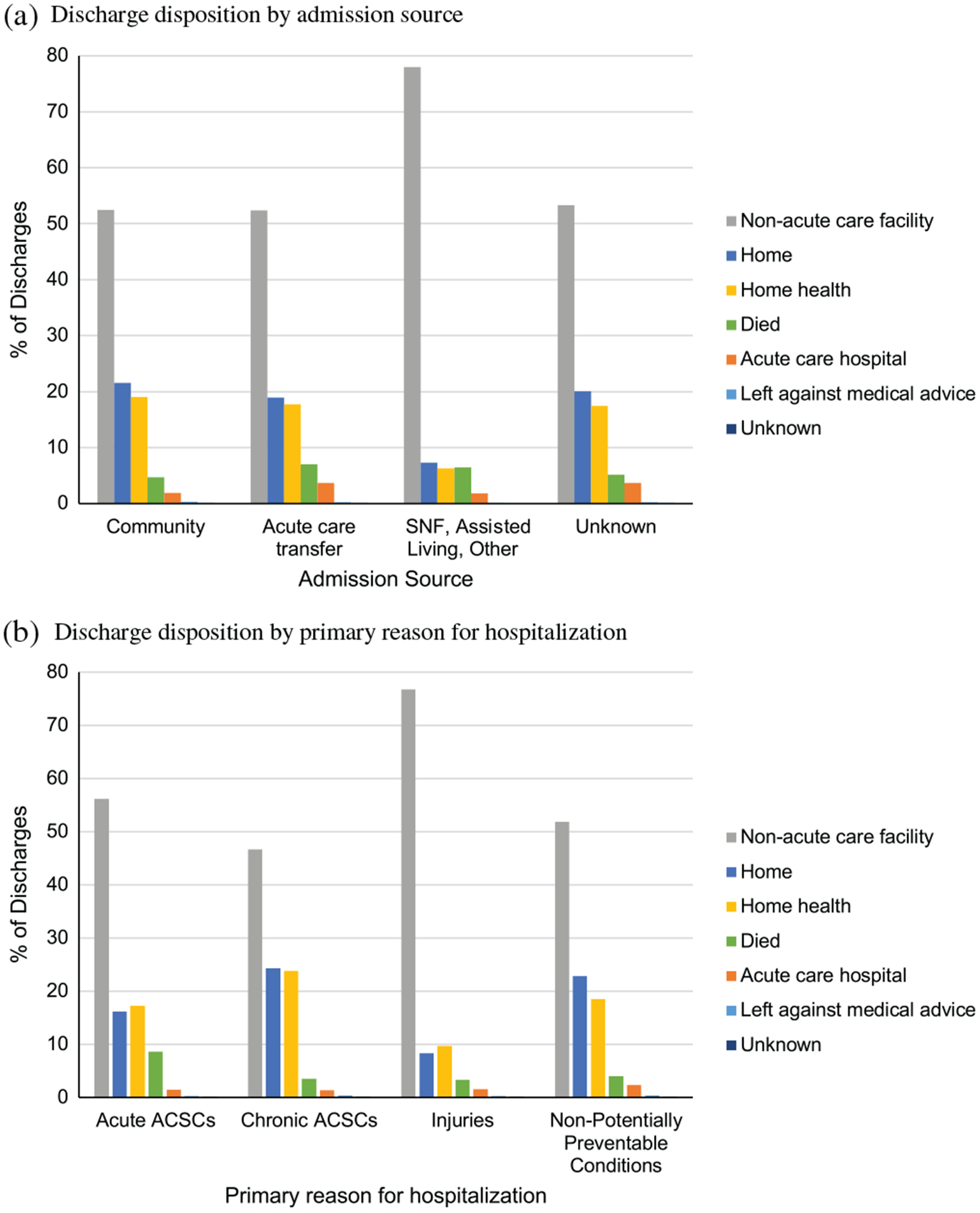
Results: The survey weighted sample represented an estimated 9.27 million hospitalizations for patients with diagnosed dementia (mean [standard deviation] age = 82.6 [6.7] years; 61.4% female). In total, 3.72 million hospitalizations were for potentially preventable conditions (40.1%), 2.07 million for acute ACSCs, .76 million for chronic ACSCs, and .89 million for injuries. Between 2012 and 2016, the incidence of all-cause hospitalizations declined from 1.87 million to 1.85 million per year (P = .04) while the incidence of potentially preventable hospitalizations increased from .75 million to .87 million per year (P < .001), driven by an increased number of hospitalizations of community-dwelling older adults. Among patients with dementia hospitalized for potentially preventable conditions, inpatient mortality declined from 6.4% to 6.1% (P < .001), inflation-adjusted median costs increased from $7,319 to $7,543 (P < .001), and total annual costs increased from $7.4 to $9.3 billion. Although 86.0% of hospitalized patients were admitted from the community, only 32.7% were discharged to the community.
Conclusion: The number of potentially preventable hospitalizations of older adults with dementia is increasing, driven by hospitalizations of community-dwelling older adults. Improved strategies for early detection and goal-directed treatment of potentially preventable conditions in patients with dementia are urgently needed. J Am Geriatr Soc 68:2240-2248, 2020.
Keywords: dementia; healthcare utilization; hospitalization.
© 2020 The American Geriatrics Society.
Conflict of interest statement
Figures
References
-
- Feng Z, Coots LA, Kaganova Y, Wiener JM. Hospital and ED use among Medicare beneficiaries with dementia varies by setting and proximity to death. Health Aff (Millwood). 2014;33(4):683–690. - PubMed
-
- Bynum JP, Rabins PV, Weller W, Niefeld M, Anderson GF, Wu AW. The relationship between a dementia diagnosis, chronic illness, Medicare expenditures, and hospital use. J Am Geriatr Soc. 2004;52(2):187–194. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
