

Association of Initial Illness Severity and Outcomes After Cardiac Arrest With Targeted Temperature Management at 36 °C or 33 °C
- PMID: 32701158
- PMCID: PMC7378753
- DOI: 10.1001/jamanetworkopen.2020.8215
Association of Initial Illness Severity and Outcomes After Cardiac Arrest With Targeted Temperature Management at 36 °C or 33 °C
Abstract
Importance: It is uncertain what the optimal target temperature is for targeted temperature management (TTM) in patients who are comatose following cardiac arrest.
Objective: To examine whether illness severity is associated with changes in the association between target temperature and patient outcome.
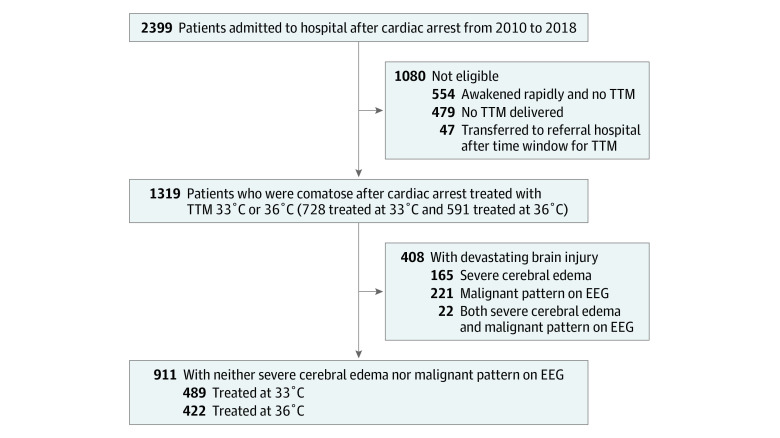
Design, setting, and participants: This cohort study compared outcomes for 1319 patients who were comatose after cardiac arrest at a single center in Pittsburgh, Pennsylvania, from January 2010 to December 2018. Initial illness severity was based on coma and organ failure scores, presence of severe cerebral edema, and presence of highly malignant electroencephalogram (EEG) after resuscitation.
Exposure: TTM at 36 °C or 33 °C.
Main outcomes and measures: Primary outcome was survival to hospital discharge, and secondary outcomes were modified Rankin Scale and cerebral performance category.
Results: Among 1319 patients, 728 (55.2%) had TTM at 33 °C (451 [62.0%] men; median [interquartile range] age, 61 [50-72] years) and 591 (44.8%) had TTM at 36 °C (353 [59.7%] men; median [interquartile range] age, 59 [48-69] years). Overall, 184 of 187 patients (98.4%) with severe cerebral edema died and 234 of 243 patients (96.3%) with highly malignant EEG died regardless of TTM strategy. Comparing TTM at 33 °C with TTM at 36 °C in 911 patients (69.1%) with neither severe cerebral edema nor highly malignant EEG, survival was lower in patients with mild to moderate coma and no shock (risk difference, -13.8%; 95% CI, -24.4% to -3.2%) but higher in patients with mild to moderate coma and cardiopulmonary failure (risk difference, 21.8%; 95% CI, 5.4% to 38.2%) or with severe coma (risk difference, 9.7%; 95% CI, 4.0% to 15.3%). Interactions were similar for functional outcomes. Most deaths (633 of 968 [65.4%]) resulted after withdrawal of life-sustaining therapies.
Conclusions and relevance: In this study, TTM at 33 °C was associated with better survival than TTM at 36 °C among patients with the most severe post-cardiac arrest illness but without severe cerebral edema or malignant EEG. However, TTM at 36 °C was associated with better survival among patients with mild- to moderate-severity illness.
Conflict of interest statement
Figures
Comment in
-
Moving Beyond One-Size-Fits-All Treatment for Patients After Cardiac Arrest.JAMA Netw Open. 2020 Jul 1;3(7):e208809. doi: 10.1001/jamanetworkopen.2020.8809. JAMA Netw Open. 2020. PMID: 32701153 No abstract available.
References
-
- Elmer J, Torres C, Aufderheide TP, et al. ; Resuscitation Outcomes Consortium . Association of early withdrawal of life-sustaining therapy for perceived neurological prognosis with mortality after cardiac arrest. Resuscitation. 2016;102:127-135. doi:10.1016/j.resuscitation.2016.01.016 - DOI - PMC - PubMed
