

Distinct clinical and immunological features of SARS-CoV-2-induced multisystem inflammatory syndrome in children
- PMID: 32701511
- PMCID: PMC7598077
- DOI: 10.1172/JCI141113
Distinct clinical and immunological features of SARS-CoV-2-induced multisystem inflammatory syndrome in children
Abstract
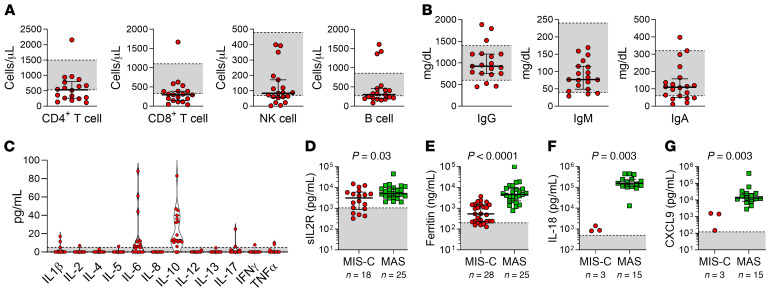
BACKGROUNDPediatric SARS-CoV-2 infection can be complicated by a dangerous hyperinflammatory condition termed multisystem inflammatory syndrome in children (MIS-C). The clinical and immunologic spectrum of MIS-C and its relationship to other inflammatory conditions of childhood have not been studied in detail.METHODSWe retrospectively studied confirmed cases of MIS-C at our institution from March to June 2020. The clinical characteristics, laboratory studies, and treatment response were collected. Data were compared with historic cohorts of Kawasaki disease (KD) and macrophage activation syndrome (MAS).RESULTSTwenty-eight patients fulfilled the case definition of MIS-C. Median age at presentation was 9 years (range: 1 month to 17 years); 50% of patients had preexisting conditions. All patients had laboratory confirmation of SARS-CoV-2 infection. Seventeen patients (61%) required intensive care, including 7 patients (25%) who required inotrope support. Seven patients (25%) met criteria for complete or incomplete KD, and coronary abnormalities were found in 6 cases. Lymphopenia, thrombocytopenia, and elevation in inflammatory markers, D-dimer, B-type natriuretic peptide, IL-6, and IL-10 levels were common but not ubiquitous. Cytopenias distinguished MIS-C from KD and the degree of hyperferritinemia and pattern of cytokine production differed between MIS-C and MAS. Immunomodulatory therapy given to patients with MIS-C included intravenous immune globulin (IVIG) (71%), corticosteroids (61%), and anakinra (18%). Clinical and laboratory improvement were observed in all cases, including 6 cases that did not require immunomodulatory therapy. No mortality was recorded in this cohort.CONCLUSIONMIS-C encompasses a broad phenotypic spectrum with clinical and laboratory features distinct from KD and MAS.FUNDINGThis work was supported by the National Institutes of Health, National Institute of Arthritis and Musculoskeletal and Skin Diseases; the National Institute of Allergy and Infectious Diseases; Rheumatology Research Foundation Investigator Awards and Medical Education Award; Boston Children's Hospital Faculty Career Development Awards; the McCance Family Foundation; and the Samara Jan Turkel Center.
Keywords: COVID-19; Clinical practice; Immunology.
Conflict of interest statement
Figures

Comment in
-
Is multisystem inflammatory syndrome in children on the Kawasaki syndrome spectrum?J Clin Invest. 2020 Nov 2;130(11):5681-5684. doi: 10.1172/JCI141718. J Clin Invest. 2020. PMID: 32730226 Free PMC article.
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
