

Chest ultrasonography versus supine chest radiography for diagnosis of pneumothorax in trauma patients in the emergency department
- PMID: 32702777
- PMCID: PMC7390330
- DOI: 10.1002/14651858.CD013031.pub2
Chest ultrasonography versus supine chest radiography for diagnosis of pneumothorax in trauma patients in the emergency department
Abstract
Background: Chest X-ray (CXR) is a longstanding method for the diagnosis of pneumothorax but chest ultrasonography (CUS) may be a safer, more rapid, and more accurate modality in trauma patients at the bedside that does not expose the patient to ionizing radiation. This may lead to improved and expedited management of traumatic pneumothorax and improved patient safety and clinical outcomes.
Objectives: To compare the diagnostic accuracy of chest ultrasonography (CUS) by frontline non-radiologist physicians versus chest X-ray (CXR) for diagnosis of pneumothorax in trauma patients in the emergency department (ED). To investigate the effects of potential sources of heterogeneity such as type of CUS operator (frontline non-radiologist physicians), type of trauma (blunt vs penetrating), and type of US probe on test accuracy.
Search methods: We conducted a comprehensive search of the following electronic databases from database inception to 10 April 2020: Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, MEDLINE, Embase, Cumulative Index to Nursing and Allied Health Literature (CINAHL) Plus, Database of Abstracts of Reviews of Effects, Web of Science Core Collection and Clinicaltrials.gov. We handsearched reference lists of included articles and reviews retrieved via electronic searching; and we carried out forward citation searching of relevant articles in Google Scholar and looked at the "Related articles" on PubMed.
Selection criteria: We included prospective, paired comparative accuracy studies comparing CUS performed by frontline non-radiologist physicians to supine CXR in trauma patients in the emergency department (ED) suspected of having pneumothorax, and with computed tomography (CT) of the chest or tube thoracostomy as the reference standard.
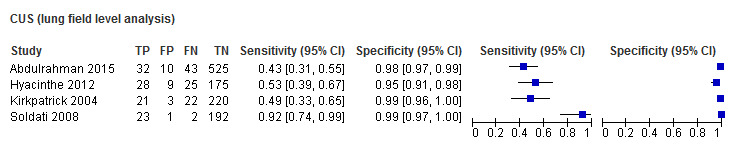
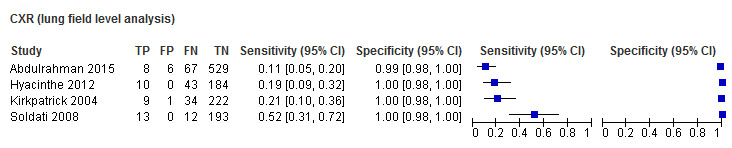
Data collection and analysis: Two review authors independently extracted data from each included study using a data extraction form. We included studies using patients as the unit of analysis in the main analysis and we included those using lung fields in the secondary analysis. We performed meta-analyses by using a bivariate model to estimate and compare summary sensitivities and specificities.
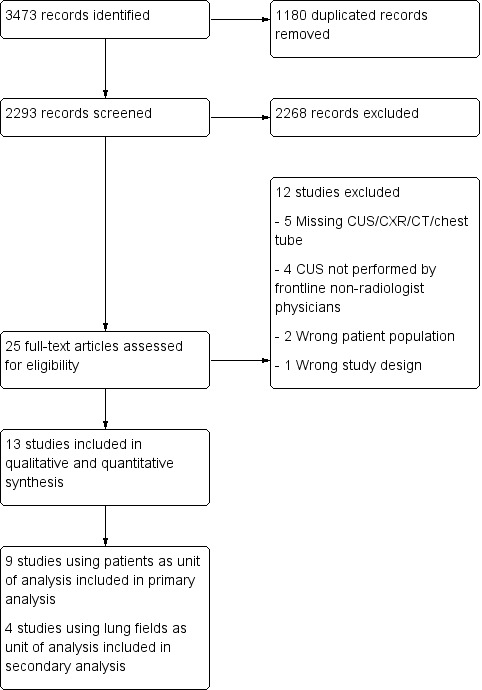
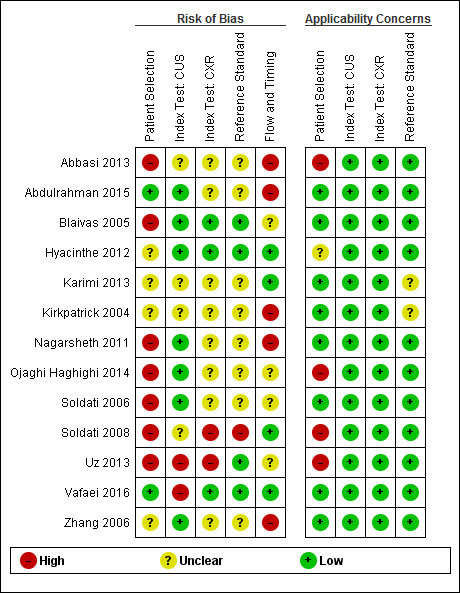
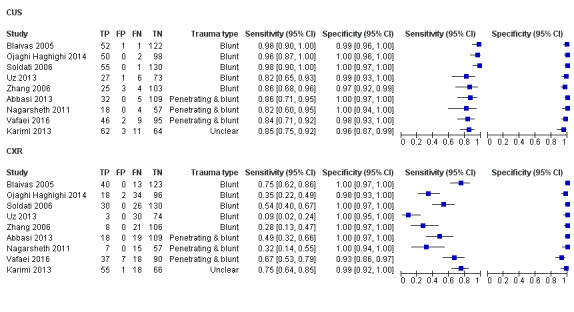
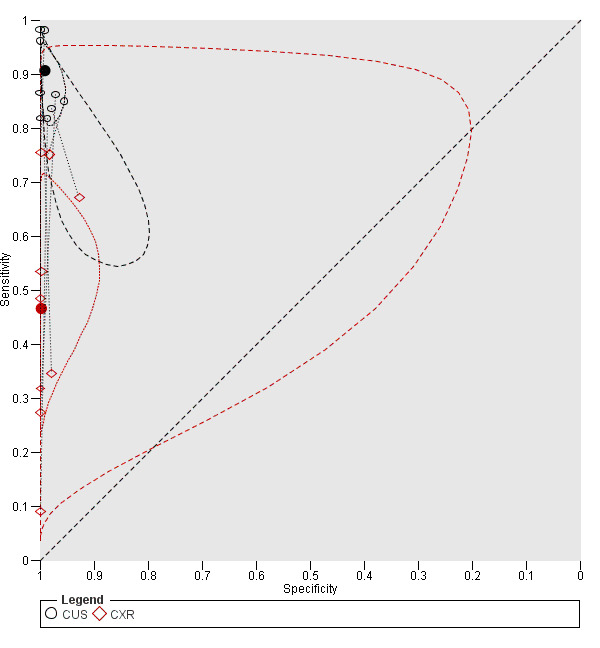
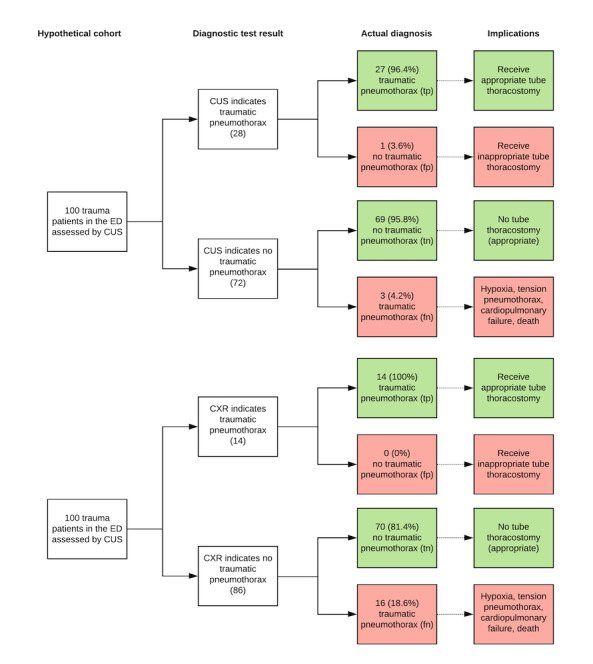
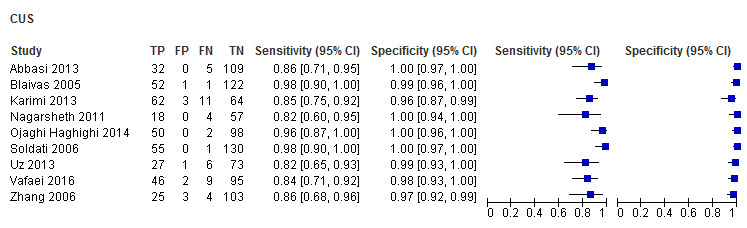
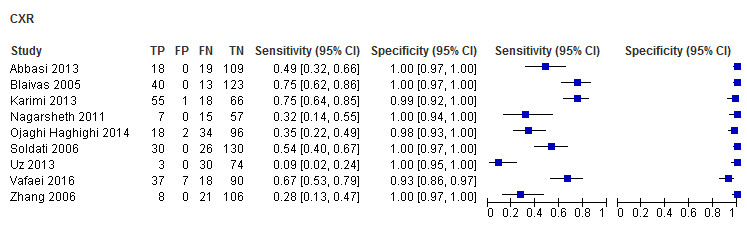
Main results: We included 13 studies of which nine (410 traumatic pneumothorax patients out of 1271 patients) used patients as the unit of analysis; we thus included them in the primary analysis. The remaining four studies used lung field as the unit of analysis and we included them in the secondary analysis. We judged all studies to be at high or unclear risk of bias in one or more domains, with most studies (11/13, 85%) being judged at high or unclear risk of bias in the patient selection domain. There was substantial heterogeneity in the sensitivity of supine CXR amongst the included studies. In the primary analysis, the summary sensitivity and specificity of CUS were 0.91 (95% confidence interval (CI) 0.85 to 0.94) and 0.99 (95% CI 0.97 to 1.00); and the summary sensitivity and specificity of supine CXR were 0.47 (95% CI 0.31 to 0.63) and 1.00 (95% CI 0.97 to 1.00). There was a significant difference in the sensitivity of CUS compared to CXR with an absolute difference in sensitivity of 0.44 (95% CI 0.27 to 0.61; P < 0.001). In contrast, CUS and CXR had similar specificities: comparing CUS to CXR, the absolute difference in specificity was -0.007 (95% CI -0.018 to 0.005, P = 0.35). The findings imply that in a hypothetical cohort of 100 patients if 30 patients have traumatic pneumothorax (i.e. prevalence of 30%), CUS would miss 3 (95% CI 2 to 4) cases (false negatives) and overdiagnose 1 (95% CI 0 to 2) of those without pneumothorax (false positives); while CXR would miss 16 (95% CI 11 to 21) cases with 0 (95% CI 0 to 2) overdiagnosis of those who do not have pneumothorax.
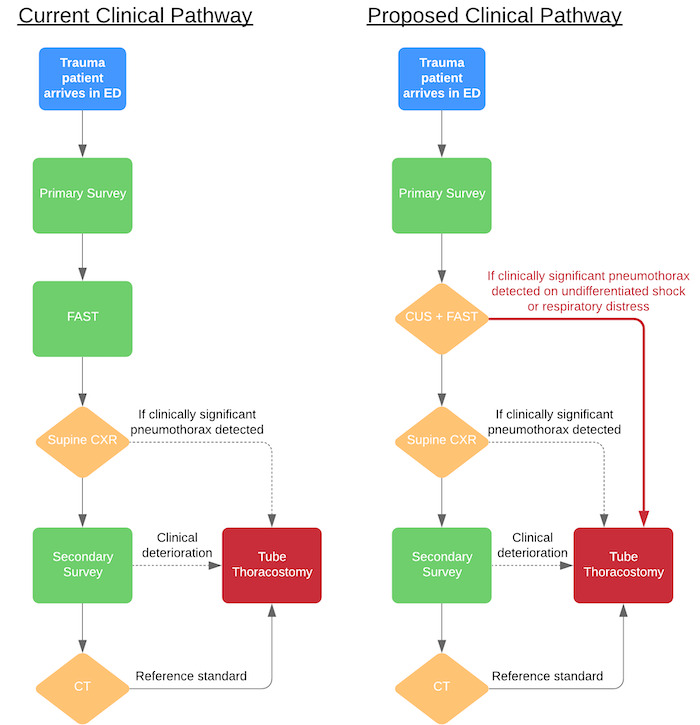
Authors' conclusions: The diagnostic accuracy of CUS performed by frontline non-radiologist physicians for the diagnosis of pneumothorax in ED trauma patients is superior to supine CXR, independent of the type of trauma, type of CUS operator, or type of CUS probe used. These findings suggest that CUS for the diagnosis of traumatic pneumothorax should be incorporated into trauma protocols and algorithms in future medical training programmes; and that CUS may beneficially change routine management of trauma.
Copyright © 2020 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
Kenneth K Chan is an Attending Emergency Physician with the University of Calgary and Alberta Health Services. He is also an Attending Emergency Physician with the University of British Columbia and Fraser Health Authority. He has no conflicts of interest to declare.
Daniel A Joo is an Attending Emergency Physician with the University of Calgary and Alberta Health Services. He has no conflicts of interest to declare.
Andrew D McRae is an Assistant Professor of Emergency Medicine and Community Health Sciences at the University of Calgary. His institution has been awarded research grants and consulting fees on cardiac biomarkers from Roche Diagnostics Canada.
Yemisi Takwoingi is a Professor of Test Evaluation and Evidence Synthesis, University of Birmingham, UK. She has no conflicts of interest to declare.
Zahra A Premji is a Research and Learning Librarian with the University of Calgary. She has no conflicts of interest to declare.
Eddy Lang is the Department Head of Emergency Medicine and a Clinician Scientist with the University of Calgary and Alberta Health Services. He has no conflicts of interest to declare.
Abel Wakai is the Director of Emergency Care Research Unit, Division of Population Health Sciences, Royal College of Surgeons, in Ireland. He has no conflicts of interest to declare.
Figures
Comment in
-
Chest ultrasonography by frontline physicians is more sensitive than CXR for diagnosing pneumothorax in trauma patients.Ann Intern Med. 2020 Nov 17;173(10):JC58. doi: 10.7326/ACPJ202011170-058. Ann Intern Med. 2020. PMID: 33197354
References
References to studies included in this review
Abbasi 2013 {published data only}
Abdulrahman 2015 {published data only}
Blaivas 2005 {published data only}
Hyacinthe 2012 {published data only}
Karimi 2013 {published data only}
-
- Karimi E, Safari S, Shekarchi B. Evaluation of the accuracy of portable ultrasound (eFAST) for detection of pneumothorax. Annals of Military and Health Sciences Research 2013;11(3):e65630.
Kirkpatrick 2004 {published data only}
-
- Kirkpatrick AW, Sirois M, Laupland KB, Liu D, Rowan K, Ball CG, et al. Hand-held thoracic sonography for detecting post-traumatic pneumothoraces: the extended focused assessment with sonography for trauma (EFAST). Journal of Trauma 2004;57(2):288-95. [DOI: 10.1097/01.TA.0000133565.88871.E4] [PMID: ] - DOI - PubMed
Nagarsheth 2011 {published data only}
-
- Nagarsheth K, Kurek S. Ultrasound detection of pneumothorax compared with chest X-ray and computed tomography scan. American Surgeon 2011;77(4):480-4. [PMID: ] - PubMed
Ojaghi Haghighi 2014 {published data only}
Soldati 2006 {published data only}
Soldati 2008 {published data only}
Uz 2013 {published and unpublished data}
-
- Uz I, Yürüktümen A, Boydak B, Bayraktaroğlu S, Ozçete E, Cevrim O, et al. Impact of the practice of "Extended Focused Assessment with Sonography for Trauma" (e-FAST) on clinical decision in the emergency department. Ulusal Travma Dergisi [Turkish Journal of Trauma & Emergency Surgery : TJTES] 2013;19(4):327-32. [DOI: 10.5505/tjtes.2013.23326] [PMID: ] - DOI - PubMed
Vafaei 2016 {published data only}
References to studies excluded from this review
Abdalla 2016 {published data only}
Agarwal 2017 {published data only}
-
- Agarwal N, Kansal HM. Chest ultrasound in the diagnosis of pneumothorax - A prospective study. Indian Journal of Public Health Research and Development 2017;8(1):275-9. [DOI: 10.5958/0976-5506.2017.00055.9] - DOI
Donmez 2012 {published data only}
Ezzat 2018 {published data only}
-
- Ezzat H, Elkahwagy M, Eltomey M, Sabry M. Evaluation of the role of bedside ultrasonography in the detection of traumatic occult pneumothorax. Journal of the Egyptian Society of Cardio-Thoracic Surgery 2018;26(2):146-50. [DOI: 10.1016/j.jescts.2018.04.004] - DOI
Heydari 2014 {published data only}
Kaya 2015 {published data only}
-
- Kaya S, Cevik AA, Acar N, Doner E, Sivrikoz C, Ozkan R. A study on the evaluation of pneumothorax by imaging methods in patients presenting to the emergency department for blunt thoracic trauma. Turkish Journal of Trauma & Emergency Surgery 2015;21(5):366-72. [DOI: 10.5505/tjtes.2015.91650] [PMID: ] - DOI - PubMed
Ku 2013 {published data only}
Mumtaz 2016 {published data only}
-
- Mumtaz U, Zahur Z, Chaudhry MA, Warraich RA. Bedside ultrasonography: a useful tool for traumatic pneumothorax. Journal of the College of Physicians and Surgeons Pakistan 2016;26(6):459-62. [PMID: ] - PubMed
Nandipati 2011 {published data only}
-
- Nandipati KC, Allamaneni S, Kakarla R, Wong A, Richards N, Satterfield J, et al. Extended focused assessment with sonography for trauma (EFAST) in the diagnosis of pneumothorax: experience at a community based level I trauma center. Injury 2011;42(5):511-4. [DOI: 10.1016/j.injury.2010.01.105] [PMID: ] - DOI - PubMed
Subramaniam 2017 {published data only}
-
- Subramaniam C, Chakaravarthy DA. Utility of extended focused assessment with sonography in blunt chest trauma - its clinical implication and its sensitivity compared with chest x-ray and clinical examination. Journal of Evolution of Medical and Dental Sciences 2017;6(4):328-33. [DOI: 10.14260/jemds/2017/73] - DOI
Ziapour 2015 {published data only}
-
- Ziapour B, Haji HS. "Anterior convergent" chest probing in rapid ultrasound transducer positioning versus formal chest ultrasonography to detect pneumothorax during the primary survey of hospital trauma patients: a diagnostic accuracy study. Journal of Trauma Management and Outcomes 2015;9:9. [DOI: 10.1186/s13032-015-0030-5] [PMID: ] - DOI - PMC - PubMed
Additional references
Alrajab 2013
Alrajhi 2012
ATLS 2012
-
- ATLS Committee. Advanced Trauma Life Support® Student Course Manual. 9th edition. Chicago: American College of Surgeons, 2012. [ISBN 13: 978-1-880696-02-6]
Ball 2012
Chan 2003
-
- Chan SS. Emergency bedside ultrasound to detect pneumothorax. Academic Emergency Medicine 2003;10(1):91-4. [PMID: ] - PubMed
Chu 2006
-
- Chu H, Cole SR. Bivariate meta-analysis of sensitivity and specificity with sparse data: a generalized linear mixed model approach. Journal of Clinical Epidemiology 2006;59(12):1331-2; author reply 1332-3. [PMID: ] - PubMed
Chung 2005
Chung 2014
De Vet 2013
-
- Vet HCW, Eisinga A, Riphagen II, Aertgeerts B, Pewsner D. Chapter 7: Searching for studies. In: Deeks JJ, Bossuyt PM, Gatsonis C, editor(s). Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy. Version 1.0.0. Cochrane Collaboration, 2013. Available from srdta.cochrane.org.
Ding 2011
Ebrahimi 2014
Enderson 1993
Filosso 2017
Husain 2012
Khandhar 2007
Kirkpatrick 2013
-
- Kirkpatrick AW, Rizoli S, Ouellet JF, Roberts DJ, Sirois M, Ball CG, et al. Occult pneumothoraces in critical care: a prospective multicenter randomized controlled trial of pleural drainage for mechanically ventilated trauma patients with occult pneumothoraces. Journal of Trauma and Acute Care Surgery 2013;74(3):747-54. [DOI: 10.1097/TA.0b013e3182827158] [PMID: ] - DOI - PubMed
Kwaitt 2014
Lichtenstein 2005
-
- Lichtenstein DA, Mezière G, Lascols N, Biderman P, Courret J, Gepner A, et al. Ultrasound diagnosis of occult pneumothorax. Critical Care Medicine 2005;33(6):1231-8. [PMID: ] - PubMed
Macaskill 2013
-
- Macaskill P, Gatsonis C, Deeks JJ, Harbord RM, Takwoingi Y. Chapter 10: Analysing and presenting results. In: Deeks JJ, Bossuyt PM, Gatsonis C, editor(s). Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy. Version 1.0.0. Cochrane Collaboration, 2013. Available from srdta.cochrane.org.
Mowery 2011
Noppen 2008
Reitsma 2005
-
- Reitsma JB, Glas AS, Rutjes AW, Scholten RJ, Bossuyt PM, Zwinderman AH. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews [Review]. Journal of Clinical Epidemiology 2005;58(10):982-90. [PMID: ] - PubMed
Review Manager 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rosen 2014
-
- Eckstein M, Henderson SO. Thoracic trauma. In: Marx JA, editors(s). Rosen's Emergency Medicine: Concepts and Clinical Practice. 8th edition. Vol. 1. Philadelphia: Saunders, 2014:431-58.
Sharma 2008
Shostak 2013
Stata 2017 [Computer program]
-
- Stata Statistical Software (Stata). Version 15. College Station, TX: StataCorp LLC, 2017.
Takwoingi 2013
-
- Takwoingi Y, Leeflang MM, Deeks JJ. Empirical evidence of the importance of comparative studies of diagnostic test accuracy. Annals of Internal Medicine 2013;158(7):544-54. [PMID: ] - PubMed
Takwoingi 2015a
Takwoingi 2015b
Volpicelli 2011
Volpicelli 2012
Whiting 2009
Whiting 2011
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous