

Procedural Patterns and Safety of Atrial Fibrillation Ablation: Findings From Get With The Guidelines-Atrial Fibrillation
- PMID: 32703018
- PMCID: PMC7502261
- DOI: 10.1161/CIRCEP.119.007944
Procedural Patterns and Safety of Atrial Fibrillation Ablation: Findings From Get With The Guidelines-Atrial Fibrillation
Abstract
Background: Catheter ablation is an increasingly used treatment for symptomatic atrial fibrillation (AF). However, there are limited prospective, nationwide data on patient selection and procedural characteristics. This study describes patient characteristics, techniques, treatment patterns, and safety outcomes of patients undergoing AF ablation.
Methods: A total of 3139 patients undergoing AF ablation between 2016 and 2018 in the Get With The Guidelines-Atrial Fibrillation registry from 24 US centers were included. Patient demographics, medical history, procedural details, and complications were abstracted. Differences between paroxysmal and patients with persistent AF were compared using Pearson χ2 and Wilcoxon rank-sum tests.
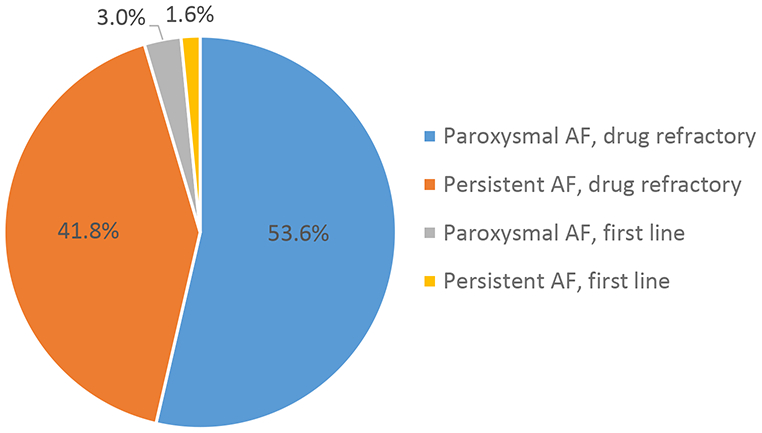
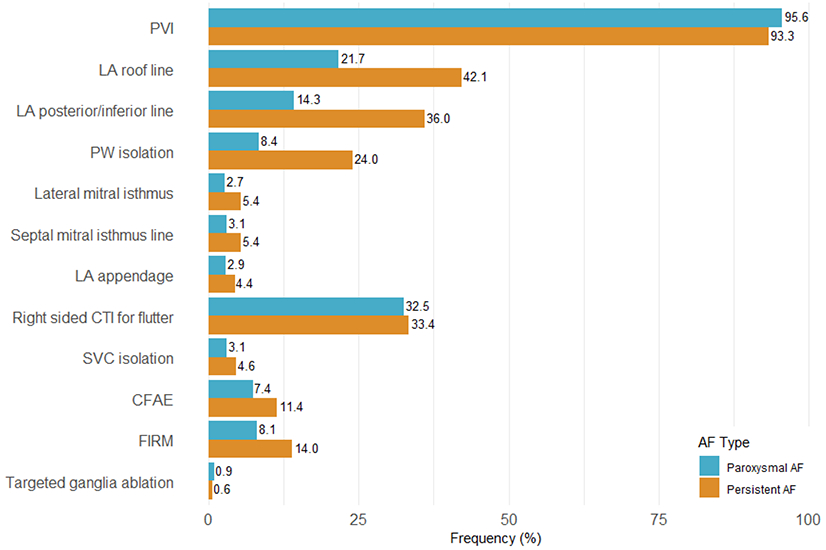
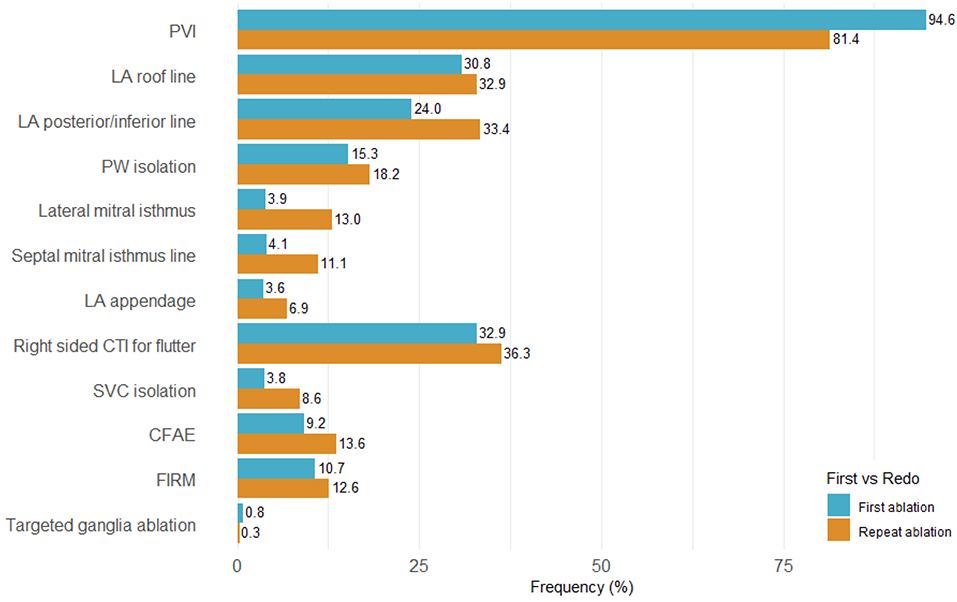
Results: Patients undergoing AF ablation were predominantly male (63.9%) and White (93.2%) with a median age of 65. Hypertension was the most common comorbidity (67.6%), and patients with persistent AF had more comorbidities than patients with paroxysmal AF. Drug refractory, paroxysmal AF was the most common ablation indication (class I, 53.6%) followed by drug refractory, persistent AF (class I, 41.8%). Radiofrequency ablation with contact force sensing was the most common ablation modality (70.5%); 23.7% of patients underwent cryoballoon ablation. Pulmonary vein isolation was performed in 94.6% of de novo ablations; the most common adjunctive lesions included left atrial roof or posterior/inferior lines, and cavotricuspid isthmus ablation. Complications were uncommon (5.1%) and were life-threatening in 0.7% of cases.
Conclusions: More than 98% of AF ablations among participating sites are performed for class I or class IIA indications. Contact force-guided radiofrequency ablation is the dominant technique and pulmonary vein isolation the principal lesion set. In-hospital complications are uncommon and rarely life-threatening.
Keywords: atrial fibrillation; catheter ablation; guideline adherence; hypertension; pulmonary vein.
Figures
References
-
- Freeman JV, Wang Y, Akar J, Desai N, Krumholz H. National Trends in Atrial Fibrillation Hospitalization, Readmission, and Mortality for Medicare Beneficiaries, 1999–2013. Circulation. 2017;135(13):1227–1239. - PubMed
-
- January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. 2014;64(21):e1–e76. - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. European heart journal. 2016;37(38):2893–2962. - PubMed
-
- Muthalaly RG, John RM, Schaeffer B, et al. Temporal trends in safety and complication rates of catheter ablation for atrial fibrillation. Journal of cardiovascular electrophysiology. 2018;29(6):854–860. - PubMed
-
- Abdur Rehman K, Wazni OM, Barakat AF, et al. Life-Threatening Complications of Atrial Fibrillation Ablation: 16-Year Experience in a Large Prospective Tertiary Care Cohort. JACC Clinical electrophysiology. 2019;5(3):284–291. - PubMed
