

Application of flexible fiberoptic bronchoscopy in the removal of adult airway foreign bodies
- PMID: 32703179
- PMCID: PMC7376862
- DOI: 10.1186/s12893-020-00825-5
Application of flexible fiberoptic bronchoscopy in the removal of adult airway foreign bodies
Abstract
Background: Flexible fiberoptic bronchoscopy is a rapid, cost effective and safe procedure.
Aim: To analyze demographic information and endoscopic findings in adult patients with airway foreign body aspiration and its removal.
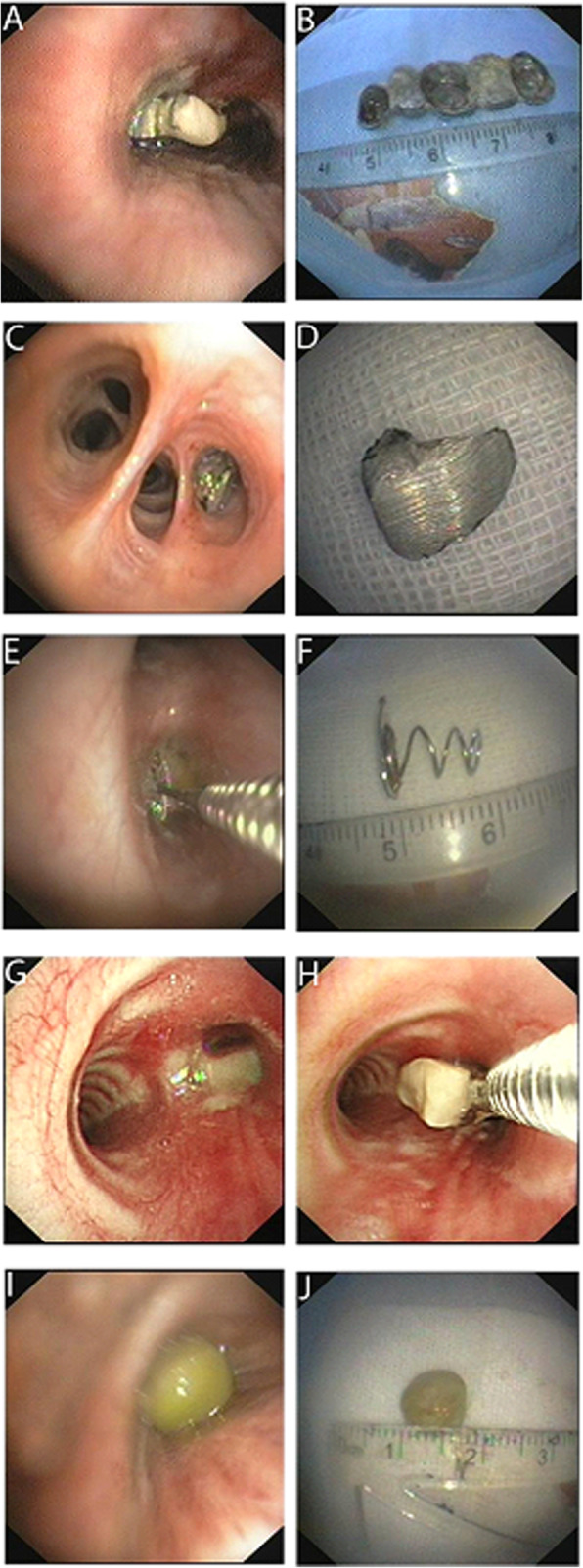
Methods: Fifty-seven adults (40 males, 17 females; average age 40 years old) with airway foreign body aspiration were analyzed. Cough (37, 65%) was the most common clinical presentation. The most common foreign body was bone followed by dental prosthesis and food debris.
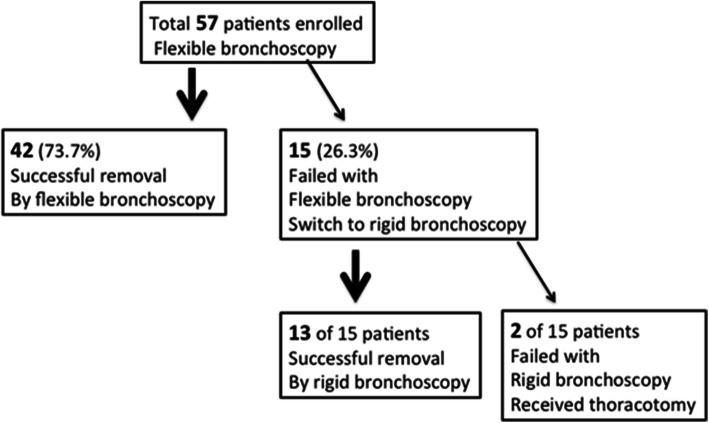
Results: In the current study, 42 out of the 57 (74%) airway foreign bodies were successfully removed under flexible fiberoptic bronchoscopy. However, it was failed in 15 patients and thus, rigid bronchoscopy was used to remove foreign bodies successfully in 13 of the 15 patients. Thoracotomy was performed for the 2 patients whose foreign body removal was unsuccessful even with rigid bronchoscopy.
Conclusion: The findings of the current study revealed that flexible fiberoptic bronchoscopy is a safe and effective procedure for the removal of adult airway foreign bodies in the majority of cases. Rigid bronchoscopy can be a backup procedure in case flexible bronchoscopy is failed.
Keywords: Adult; Airway foreign body; Flexible fiberoptic bronchoscope.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
