

Discontinuation of antidepressants after remission with antidepressant medication in major depressive disorder: a systematic review and meta-analysis
- PMID: 32704061
- PMCID: PMC7815511
- DOI: 10.1038/s41380-020-0843-0
Discontinuation of antidepressants after remission with antidepressant medication in major depressive disorder: a systematic review and meta-analysis
Abstract
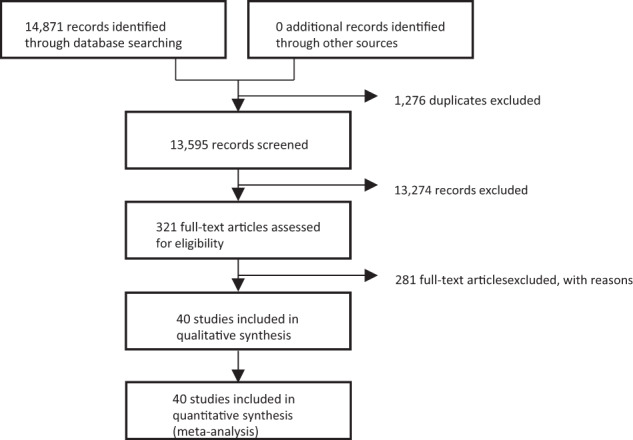
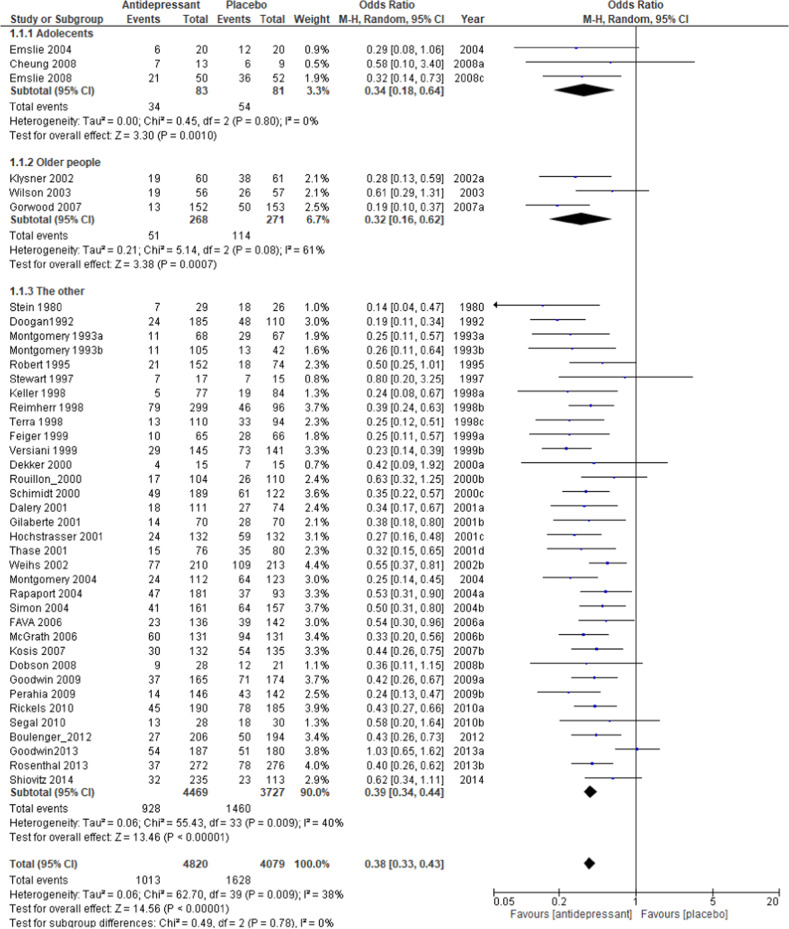
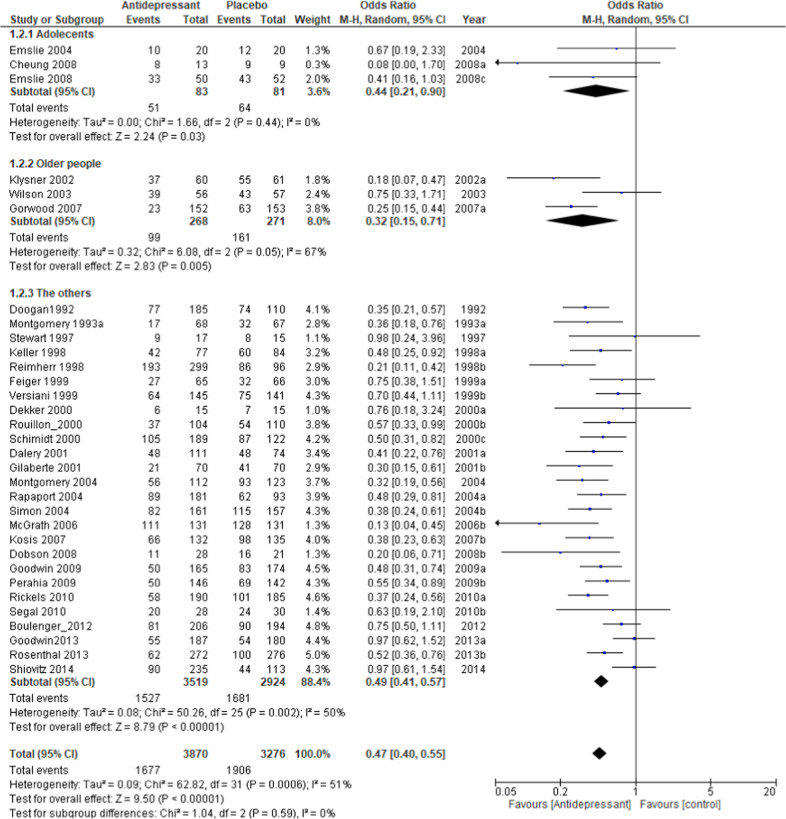
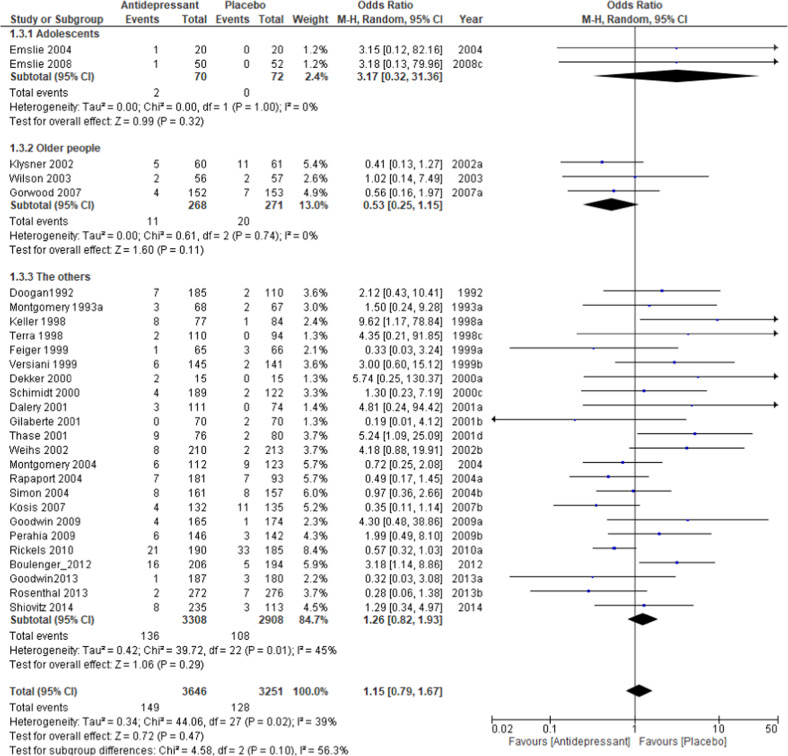
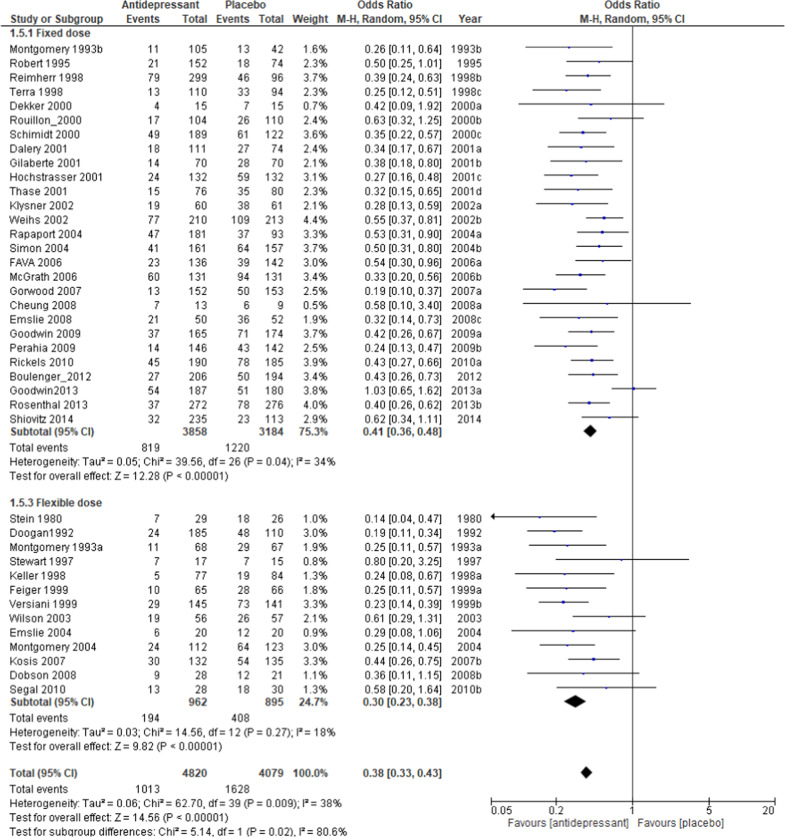
A significant clinical issue encountered after a successful acute major depressive disorder (MDD) treatment is the relapse of depressive symptoms. Although continuing maintenance therapy with antidepressants is generally recommended, there is no established protocol on whether or not it is necessary to prescribe the antidepressant used to achieve remission. In this meta-analysis, the risk of relapse and treatment failure when either continuing with the same drug used to achieved remission or switching to a placebo was assessed in several clinically significant subgroups. The pooled odds ratio (OR) (±95% confidence intervals (CI)) was calculated using a random effects model. Across 40 studies (n = 8890), the relapse rate was significantly lower in the antidepressant group than the placebo group by about 20% (OR = 0.38, CI: 0.33-0.43, p < 0.00001; 20.9% vs 39.7%). The difference in the relapse rate between the antidepressant and placebo groups was greater for tricyclics (25.3%; OR = 0.30, CI: 0.17-0.50, p < 0.00001), SSRIs (21.8%; OR = 0.33, CI: 0.28-0.38, p < 0.00001), and other newer agents (16.0%; OR = 0.44, CI: 0.36-0.54, p < 0.00001) in that order, while the effect size of acceptability was greater for SSRIs than for other antidepressants. A flexible dose schedule (OR = 0.30, CI: 0.23-0.48, p < 0.00001) had a greater effect size than a fixed dose (OR = 0.41, CI: 0.36-0.48, p < 0.00001) in comparison to placebo. Even in studies assigned after continuous treatment for more than 6 months after remission, the continued use of antidepressants had a lower relapse rate than the use of a placebo (OR = 0.40, CI: 0.29-0.55, p < 0.00001; 20.2% vs 37.2%). The difference in relapse rate was similar from a maintenance period of 6 months (OR = 0.41, CI: 0.35-0.48, p < 0.00001; 19.6% vs 37.6%) to over 1 year (OR = 0.35, CI: 0.29-0.41, p < 0.00001; 19.9% vs 39.8%). The all-cause dropout of antidepressant and placebo groups was 43% and 58%, respectively, (OR = 0.47, CI: 0.40-0.55, p < 0.00001). The tolerability rate was ~4% for both groups. The rate of relapse (OR = 0.32, CI: 0.18-0.64, p = 0.0010, 41.0% vs 66.7%) and all-cause dropout among adolescents was higher than in adults. To prevent relapse and treatment failure, maintenance therapy, and careful attention for at least 6 months after remission is recommended. SSRIs are well-balanced agents, and flexible dose adjustments are more effective for relapse prevention.
Conflict of interest statement
The authors have declared that there are no conflicts of interest in relation to the subject of this study. We have had the following interests for the past 3 years. MK has received grant funding from the Japan Society for the Promotion of Science, SENSHIN Medical Research Foundation and Japan Research Foundation for Clinical Pharmacology, and speaker’s honoraria from Sumitomo Dainippon Pharma, Otsuka, Meiji-Seika Pharma, Eli Lilly, MSD K.K., GlaxoSmithKline, Pfizer, Janssen Pharmaceutical, Shionogi, Mitsubishi Tanabe Pharma, Takeda Pharmaceutical, Lundbeck and Ono Pharmaceutical. Dr. Hori has received grant funding from Ministry of Education, Culture, Sports, Science and Technology Japan and UOEH Research Grant for Promotion of Occupational Health and speaker’s honoraria from Sumitomo Dainippon Pharma, Otsuka, Meiji-Seika Pharma, Eli Lilly, MSD K.K., Pfizer, Janssen Pharmaceutical, Shionogi, Takeda Pharmaceutical and Lundbeck. Dr. Inoue has received speaker’s honoraria from Mochida Pharmaceutical, Takeda Pharmaceutical, Eli Lilly, Janssen Pharmaceutical, MSD, Taisho Toyama Pharmaceutical, Yoshitomiyakuhin, and Daiichi Sankyo; grants from Shionogi, Astellas, Tsumura, and Eisai; grants and speaker’s honoraria from Otsuka Pharmaceutical, Dainippon Sumitomo Pharma, Mitsubishi Tanabe Pharma, Kyowa Pharmaceutical Industry, Pfizer, Novartis Pharma, and Meiji Seika Pharma; and is a member of the advisory boards of Pfizer, Novartis Pharma, and Mitsubishi Tanabe Pharma. Dr. Tajika received the lecture fee from Mitsubishi-Tanabe, Otsuka and Sumitomo Dainippon Pharma. Dr. Inagaki was employed through an endowed chair sponsored by the Government of Shiga Prefecture, Japan, from 2010 to 2016, has received grant funding from National Mutual Insurance Federation of Agricultural Cooperatives, Shionogi & Co., Ltd, Otsuka Pharmaceutical Co., Ltd, Shiga University of Medical Science and The Shiga Medical Science Association for International Cooperation and speaker’s honoraria from Japan Laim Corporation, Otsuka Pharmaceutical Co.,Ltd and Yoshitomiyakuhin Corporation. Dr. Iga has received grant funding from the Japan Society for the Promotion of Science and speaker’s honoraria from Sumitomo Dainippon Pharma, Otsuka, Meiji-Seika Pharma, Eli Lilly, MSD K.K., Novartis Pharma K.K., Sanofi K.K., Mochida Pharmaceutical, Takeda Pharmaceutical, Yoshitomiyakuhin, Eisai, Mylan, Sawai Pharmaceutical, Kyowa pharmaceutical industry, and Ono Pharmaceutical. Dr. Iwata has received grant funding from Japan Society for the Promotion Science, SENSHIN Medical Research Foundation, Japan Agency for Medical Research and Development and Osaka Gas, and speaker’s honoraria from Sumitomo Dainippon Pharma, Otsuka, Meiji-Seika Pharma, Eli Lilly, MSD K.K., Pfizer, Janssen Pharmaceutical and Mochida Pharmaceutical. Dr. Imai received the lecture fee from Tanabe-Mitsubishi pharma and Kyowa pharmaceutical industry outside the submitted work. Dr, Mishima has received research support from the Japanese Ministry of Health, Labor and Welfare (H29-Seishin-Ippan-001, 19GC1012); the Japanese Ministry of Education, Science, and Technology; and the National. Center of Neurology and Psychiatry Intramural Research Grant for Neurological and Psychiatric Disorders, and also collaborative research fund with Taisho Pharmaceutical Co., Ltd., speaker’s honoraria from Eisai Co., Ltd., MSD Inc., Takeda Pharmaceutical Co., Ltd., Astellas Pharma Inc., and Janssen Pharmaceutical along with research grants from Eisai Co., Ltd., Nobelpharma Co., Ltd., and Takeda Pharmaceutical Co., Ltd.
Figures
References
-
- Zimmerman M, Martinez JA, Attiullah N, Friedman M, Toba C, Boerescu DA, et al. Why do some depressed outpatients who are in remission according to the Hamilton Depression Rating Scale not consider themselves to be in remission? J Clin Psychiatry. 2012;73:790–5. doi: 10.4088/JCP.11m07203. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
