

Leflunomide monotherapy versus combination therapy with conventional synthetic disease-modifying antirheumatic drugs for rheumatoid arthritis: a retrospective study
- PMID: 32704073
- PMCID: PMC7378063
- DOI: 10.1038/s41598-020-69309-z
Leflunomide monotherapy versus combination therapy with conventional synthetic disease-modifying antirheumatic drugs for rheumatoid arthritis: a retrospective study
Abstract
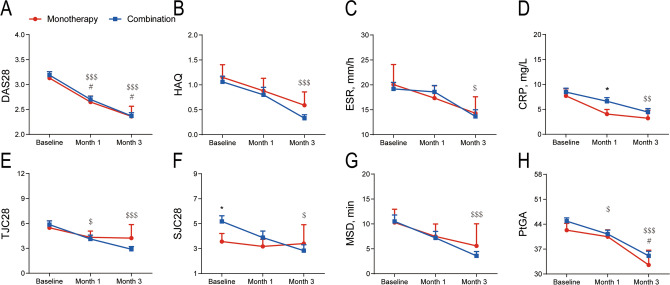
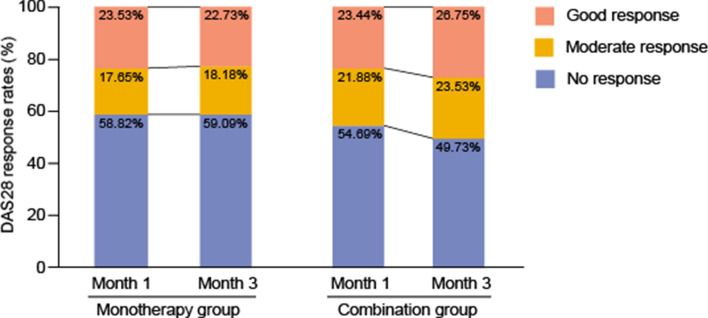
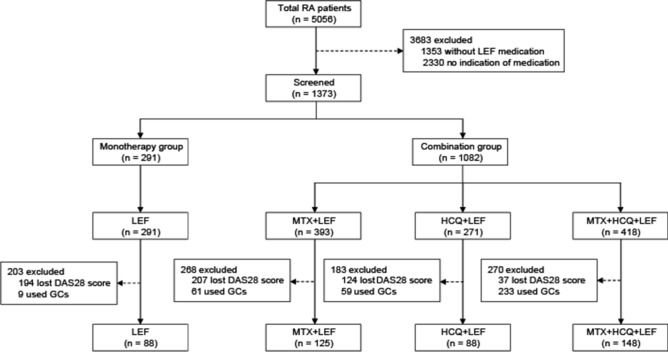
Leflunomide (LEF) is a conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) for the treatment of rheumatoid arthritis. However, there are few reports on the comparison of efficacy between LEF alone and combined with other csDMARDs. Here, the efficacy and safety of LEF monotherapy (88) and combination (361) therapy groups were evaluated. After 3 months, there were no significant differences in 28-joint disease activity score (DAS28), health assessment questionnaire (HAQ), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) between the monotherapy and combination groups (all P > 0.05). According to the European League Against Rheumatism (EULAR) response criteria, it was found that the DAS28 response rates were similar in the two groups (P > 0.05). Besides, the two groups presented similar safety profiles. Subgroup analysis found that there was no difference in efficacy among the three combined therapies (LEF + methotrexate (MTX), LEF + hydroxychloroquine (HCQ), and LEF + MTX + HCQ) and LEF monotherapy. Furthermore, when the dose of LEF was less than 40 mg/day, no significant difference in efficacy was observed between low and high doses. Overall, these results indicated that low dose LEF monotherapy was not inferior to the combination therapy.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Humphreys JH, et al. The incidence of rheumatoid arthritis in the UK: Comparisons using the 2010 ACR/EULAR classification criteria and the 1987 ACR classification criteria. Results from the Norfolk Arthritis register. Ann. Rheum. Dis. 2013;72:1315–1320. doi: 10.1136/annrheumdis-2012-201960. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
