

Thrower's Exostosis of the Shoulder: A Systematic Review With a Novel Classification
- PMID: 32704507
- PMCID: PMC7361505
- DOI: 10.1177/2325967120932101
Thrower's Exostosis of the Shoulder: A Systematic Review With a Novel Classification
Abstract
Background: A variety of thrower's exostoses are grouped under the term Bennett lesion, which makes understanding diagnosis and treatment difficult.
Purpose: To identify all types of reported thrower's and overhead athlete's exostoses and categorize them into a classification system to allow a morphology-based classification.
Study design: Systematic review; Level of evidence, 4.
Methods: A systematic review of all articles pertaining to Bennett lesions and thrower's exostosis was performed. The classification and treatments were evaluated to describe the types, proposed causes, diagnosis, and treatment options.
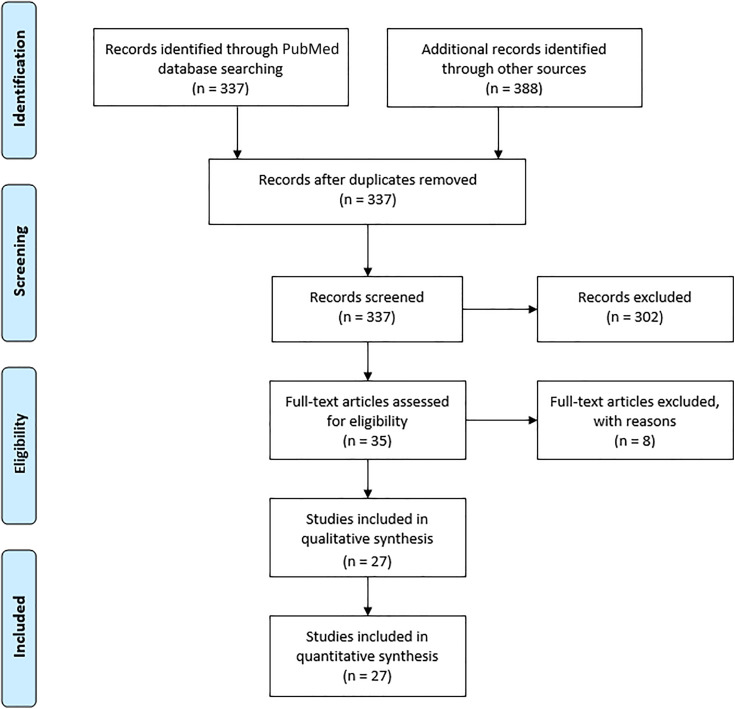
Results: A total of 27 studies were included in the systematic review. The anatomic locations referenced in the study demonstrated posteroinferior, posterior, and posterosuperior glenoid lesions. Aggregate radiographic data demonstrated 158 of 306 patients (52%) with a thrower's exostosis of any type and location. Of these 158 patients with a radiographic lesion, 119 (75%) patients were symptomatic. The locations were posteroinferior in 110 patients (70%), directly posterior in 2 patients (1.3%), posterosuperior in 44 patients (28%), and unknown in 2 patients (1.3%). Avulsed lesions were present in 9 (5.7%) posteroinferior lesions, 0 direct posterior lesions, and 2 (1.3%) posterosuperior lesions. Treatment plans included both nonoperative and operative strategies, but operative intervention was more commonly reported for detached lesions. After operative intervention, only 61% of reported athletes returned to preinjury performance.
Conclusion: Based on a comprehensive review of the literature, we identified several anatomic locations for a thrower's exostosis beyond the classic Bennett lesion. We categorized the reported exostoses into a new classification system for description of location and type (subperiosteal or free fragment) of the thrower's exostosis, which may be used to study future treatments. Current treatment strategies recommend that surgical treatment of thrower's exostosis is considered only after exhausting nonoperative management because reported return to sport is variable after surgery. The effectiveness of excision or repair for both subperiosteal and detached lesions has not been established.
Keywords: Bennett lesion; classification; glenohumeral internal rotation deficit (GIRD); overhead athlete; posterosuperior impingement; thrower’s exostosis; treatment.
© The Author(s) 2020.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: M.T.F. has received grant support from DJO, consulting fees from DePuy/Medical Device Business Services and Smith & Nephew, speaking fees from Integra and Smith & Nephew, and hospitality payments from Wright Medical. S.M. has received educational support from Arthrex, DJO, and Smith & Nephew. L.D.H. has received educational support from Arthrex and Kairos Surgical, consulting fees from Arthrex, and hospitality payments from Arthrex and Ethicon. A.V.S. has received institutional and fellowship educational grants from Arthrex, Medwest, and Smith & Nephew; consulting fees from Allosource; and hospitality payments from Stryker and Wright Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures



References
-
- Andrews JR, Dugas JR, Hackel JG, Reinold MM, Wilk KE. The thrower’s exostosis pathophysiology and management. Tech Shoulder Elbow Surg. 2004;5(1):44–50.
-
- Barnes DA, Tullos HS. An analysis of 100 symptomatic baseball players. Am J Sports Med. 1978;6(2):62–67. - PubMed
-
- Bennett DL, El-Khoury GY. Update of imaging of sports injuries to the upper extremity: shoulder and elbow. Imaging Decisions MRI. 2005;9(3):32–38.
-
- Bennett GE. Shoulder and elbow lesions of the professional baseball pitcher. JAMA. 1941;117:510–514.
Publication types
LinkOut - more resources
Full Text Sources
