

Diagnosis of Hypersensitivity Pneumonitis in Adults. An Official ATS/JRS/ALAT Clinical Practice Guideline
- PMID: 32706311
- PMCID: PMC7397797
- DOI: 10.1164/rccm.202005-2032ST
Diagnosis of Hypersensitivity Pneumonitis in Adults. An Official ATS/JRS/ALAT Clinical Practice Guideline
Erratum in
-
Erratum: Diagnosis of Hypersensitivity Pneumonitis in Adults: An Official ATS/JRS/ALAT Clinical Practice Guideline.Am J Respir Crit Care Med. 2021 Jan 1;203(1):150-151. doi: 10.1164/rccm.v203erratum1. Am J Respir Crit Care Med. 2021. PMID: 33385222 Free PMC article. No abstract available.
-
Erratum for Table 2: Diagnosis of Hypersensitivity Pneumonitis in Adults. An Official ATS/JRS/ALAT Clinical Practice Guideline.Am J Respir Crit Care Med. 2022 Aug 15;206(4):518. doi: 10.1164/rccm.v206erratum4. Am J Respir Crit Care Med. 2022. PMID: 35969192 No abstract available.
Abstract
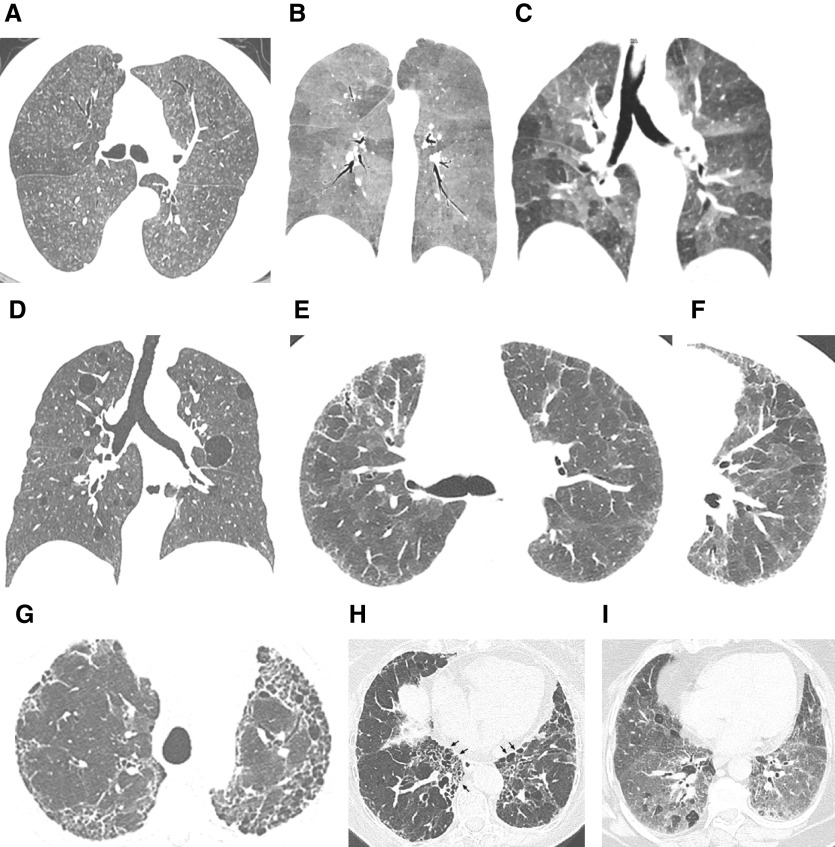
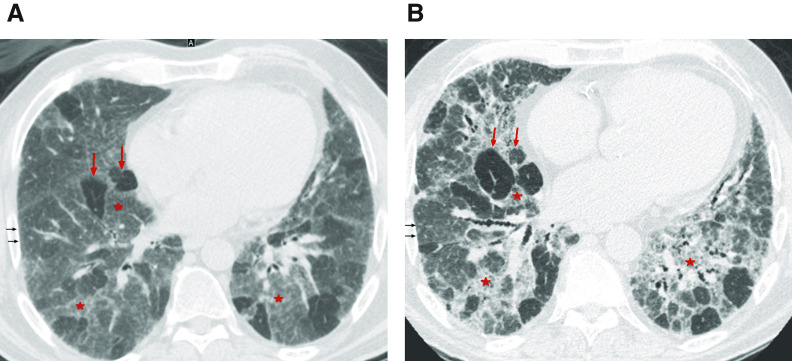
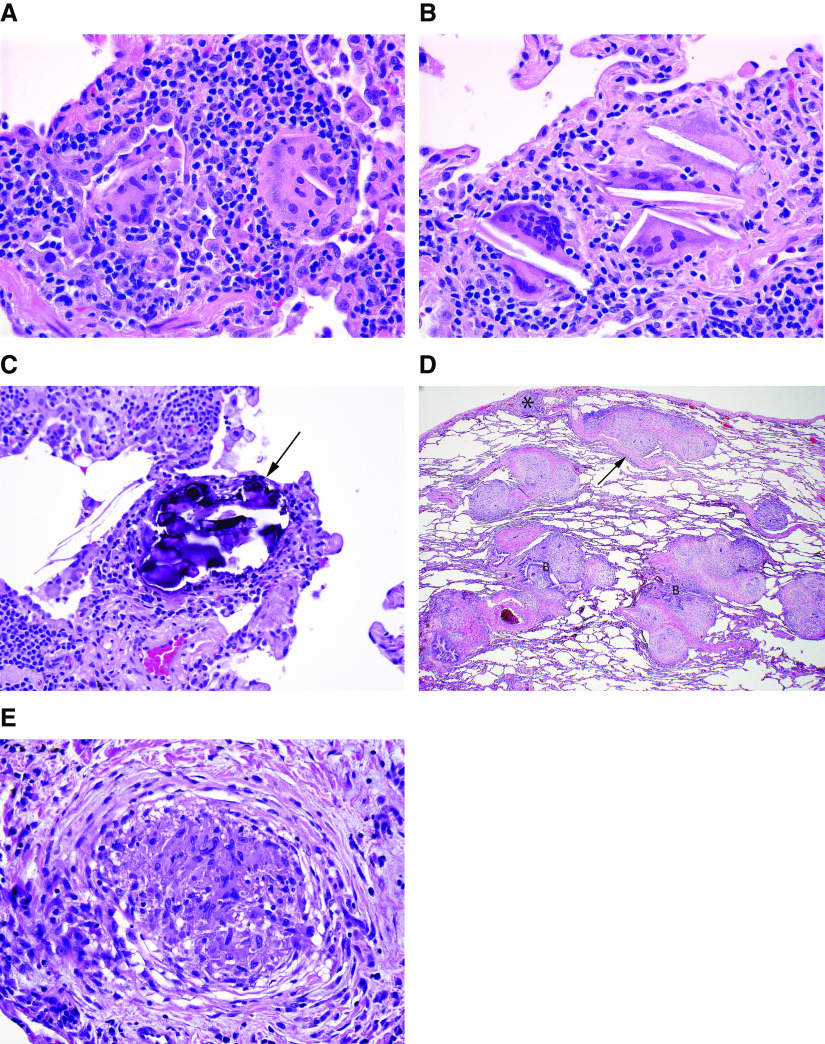
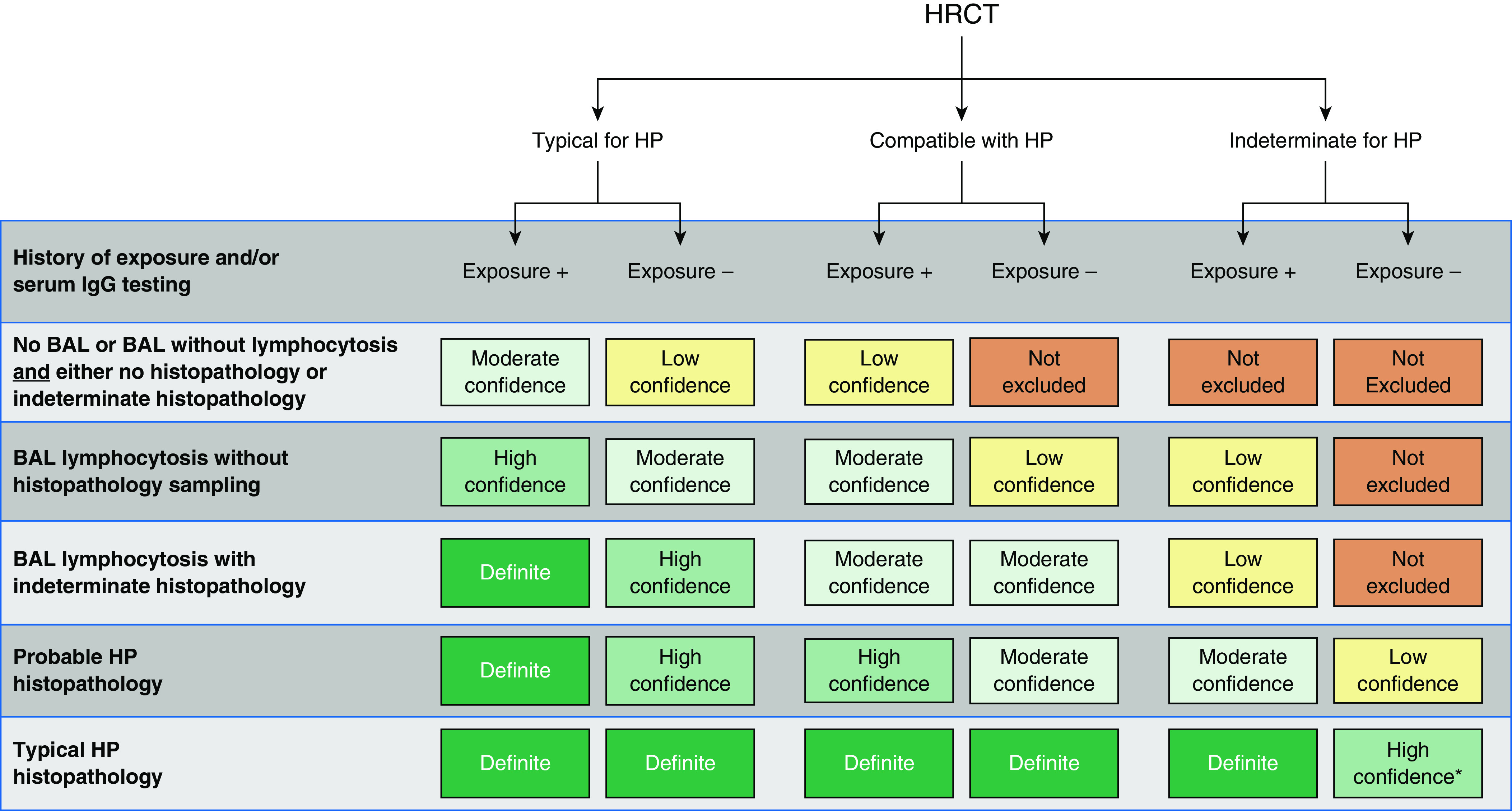
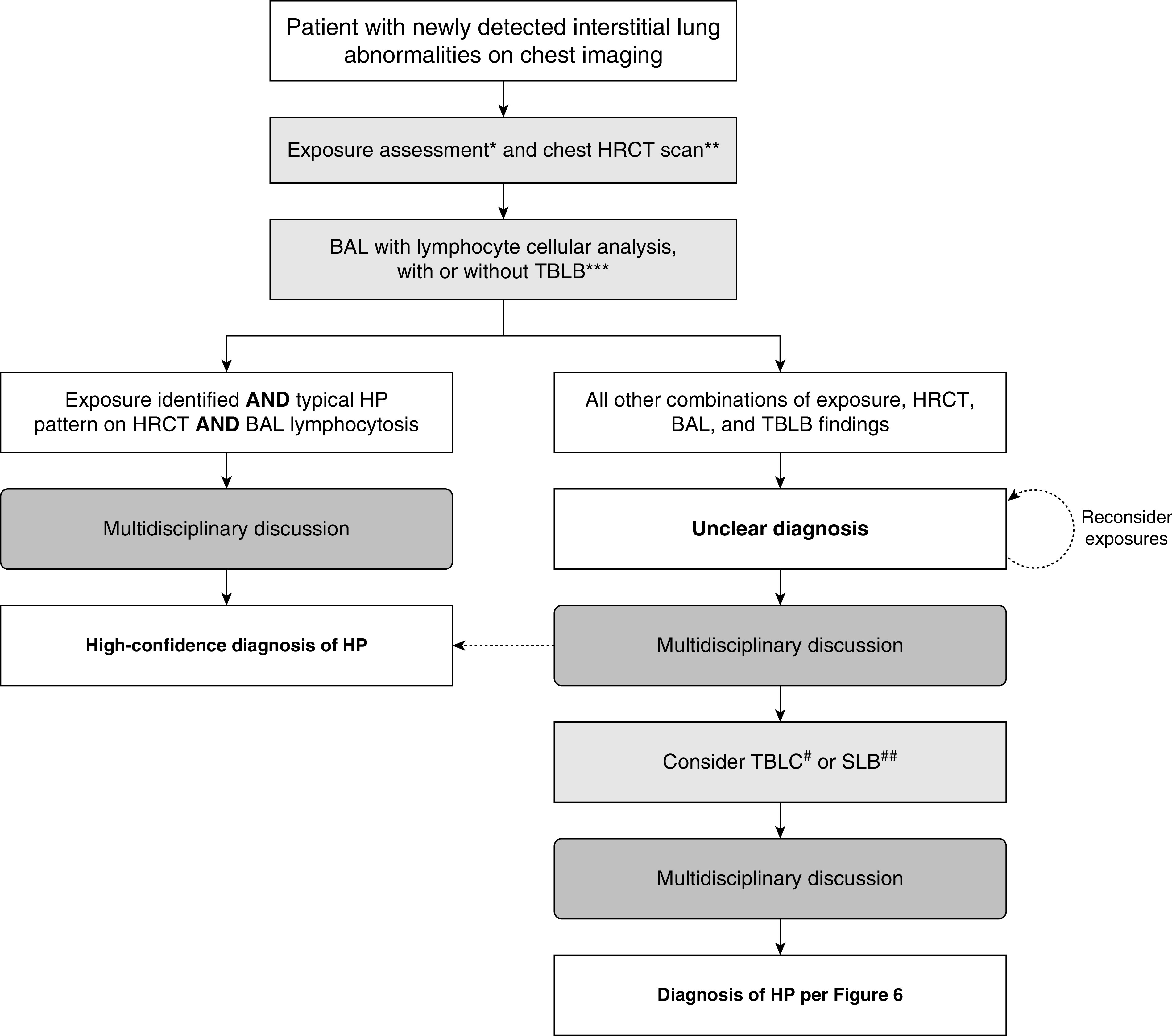
Background: This guideline addresses the diagnosis of hypersensitivity pneumonitis (HP). It represents a collaborative effort among the American Thoracic Society, Japanese Respiratory Society, and Asociación Latinoamericana del Tórax.Methods: Systematic reviews were performed for six questions. The evidence was discussed, and then recommendations were formulated by a multidisciplinary committee of experts in the field of interstitial lung disease and HP using the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) approach.Results: The guideline committee defined HP, and clinical, radiographic, and pathological features were described. HP was classified into nonfibrotic and fibrotic phenotypes. There was limited evidence that was directly applicable to all questions. The need for a thorough history and a validated questionnaire to identify potential exposures was agreed on. Serum IgG testing against potential antigens associated with HP was suggested to identify potential exposures. For patients with nonfibrotic HP, a recommendation was made in favor of obtaining bronchoalveolar lavage (BAL) fluid for lymphocyte cellular analysis, and suggestions for transbronchial lung biopsy and surgical lung biopsy were also made. For patients with fibrotic HP, suggestions were made in favor of obtaining BAL for lymphocyte cellular analysis, transbronchial lung cryobiopsy, and surgical lung biopsy. Diagnostic criteria were established, and a diagnostic algorithm was created by expert consensus. Knowledge gaps were identified as future research directions.Conclusions: The guideline committee developed a systematic approach to the diagnosis of HP. The approach should be reevaluated as new evidence accumulates.
Keywords: fibrotic hypersensitivity pneumonitis; hypersensitivity pneumonitis; interstitial lung disease; nonfibrotic hypersensitivity pneumonitis; pulmonary fibrosis.
Figures


Comment in
-
Reply to Morán-Mendoza and Khalil: Are Ground-Glass Opacities on Chest High-Resolution Computed Tomography a Manifestation of Airway Disease?Am J Respir Crit Care Med. 2021 Mar 15;203(6):781-782. doi: 10.1164/rccm.202012-4410LE. Am J Respir Crit Care Med. 2021. PMID: 33434473 Free PMC article. No abstract available.
-
Are Ground-Glass Opacities on Chest High-Resolution Computed Tomography a Manifestation of Airway Disease?Am J Respir Crit Care Med. 2021 Mar 15;203(6):780-781. doi: 10.1164/rccm.202011-4276LE. Am J Respir Crit Care Med. 2021. PMID: 33434474 Free PMC article. No abstract available.
-
Hypersensitivity Pneumonitis: Correct Identification of Causative Microbial Agents Is Essential for Efficient Diagnosis and Prevention.Am J Respir Crit Care Med. 2023 Jul 15;208(2):213-214. doi: 10.1164/rccm.202211-2182LE. Am J Respir Crit Care Med. 2023. PMID: 36693272 Free PMC article. No abstract available.
References
-
- Lacasse Y, Selman M, Costabel U, Dalphin JC, Ando M, Morell F, et al. HP Study Group. Clinical diagnosis of hypersensitivity pneumonitis. Am J Respir Crit Care Med. 2003;168:952–958. - PubMed
-
- Elicker BM, Jones KD, Henry TS, Collard HR. Multidisciplinary approach to hypersensitivity pneumonitis. J Thorac Imaging. 2016;31:92–103. - PubMed
-
- Churg A, Muller NL, Flint J, Wright JL. Chronic hypersensitivity pneumonitis. Am J Surg Pathol. 2006;30:201–208. - PubMed
-
- Fink JN, Ortega HG, Reynolds HY, Cormier YF, Fan LL, Franks TJ, et al. Needs and opportunities for research in hypersensitivity pneumonitis. Am J Respir Crit Care Med. 2005;171:792–798. - PubMed
-
- Schuyler M, Cormier Y. The diagnosis of hypersensitivity pneumonitis. Chest. 1997;111:534–536. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
