

Development of a Deep Learning Model to Identify Lymph Node Metastasis on Magnetic Resonance Imaging in Patients With Cervical Cancer
- PMID: 32706384
- PMCID: PMC7382006
- DOI: 10.1001/jamanetworkopen.2020.11625
Development of a Deep Learning Model to Identify Lymph Node Metastasis on Magnetic Resonance Imaging in Patients With Cervical Cancer
Abstract
Importance: Accurate identification of lymph node metastasis preoperatively and noninvasively in patients with cervical cancer can avoid unnecessary surgical intervention and benefit treatment planning.
Objective: To develop a deep learning model using preoperative magnetic resonance imaging for prediction of lymph node metastasis in cervical cancer.
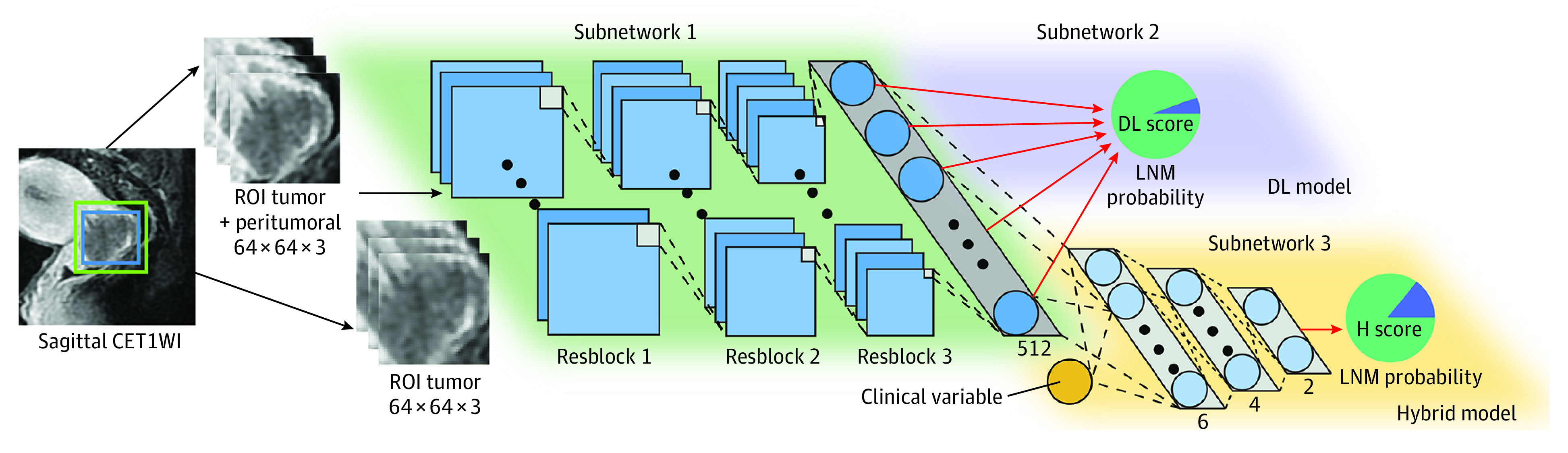
Design, setting, and participants: This diagnostic study developed an end-to-end deep learning model to identify lymph node metastasis in cervical cancer using magnetic resonance imaging (MRI). A total of 894 patients with stage IB to IIB cervical cancer who underwent radical hysterectomy and pelvic lymphadenectomy were reviewed. All patients underwent radical hysterectomy and pelvic lymphadenectomy, received pelvic MRI within 2 weeks before the operations, had no concurrent cancers, and received no preoperative treatment. To achieve the optimal model, the diagnostic value of 3 MRI sequences was compared, and the outcomes in the intratumoral and peritumoral regions were explored. To mine tumor information from both image and clinicopathologic levels, a hybrid model was built and its prognostic value was assessed by Kaplan-Meier analysis. The deep learning model and hybrid model were developed on a primary cohort consisting of 338 patients (218 patients from Sun Yat-sen University Cancer Center, Guangzhou, China, between January 2011 and December 2017 and 120 patients from Henan Provincial People's Hospital, Zhengzhou, China, between December 2016 and June 2018). The models then were evaluated on an independent validation cohort consisting of 141 patients from Yunnan Cancer Hospital, Kunming, China, between January 2011 and December 2017.
Main outcomes and measures: The primary diagnostic outcome was lymph node metastasis status, with the pathologic characteristics diagnosed by lymphadenectomy. The secondary primary clinical outcome was survival. The primary diagnostic outcome was assessed by receiver operating characteristic (area under the curve [AUC]) analysis; the primary clinical outcome was assessed by Kaplan-Meier survival analysis.
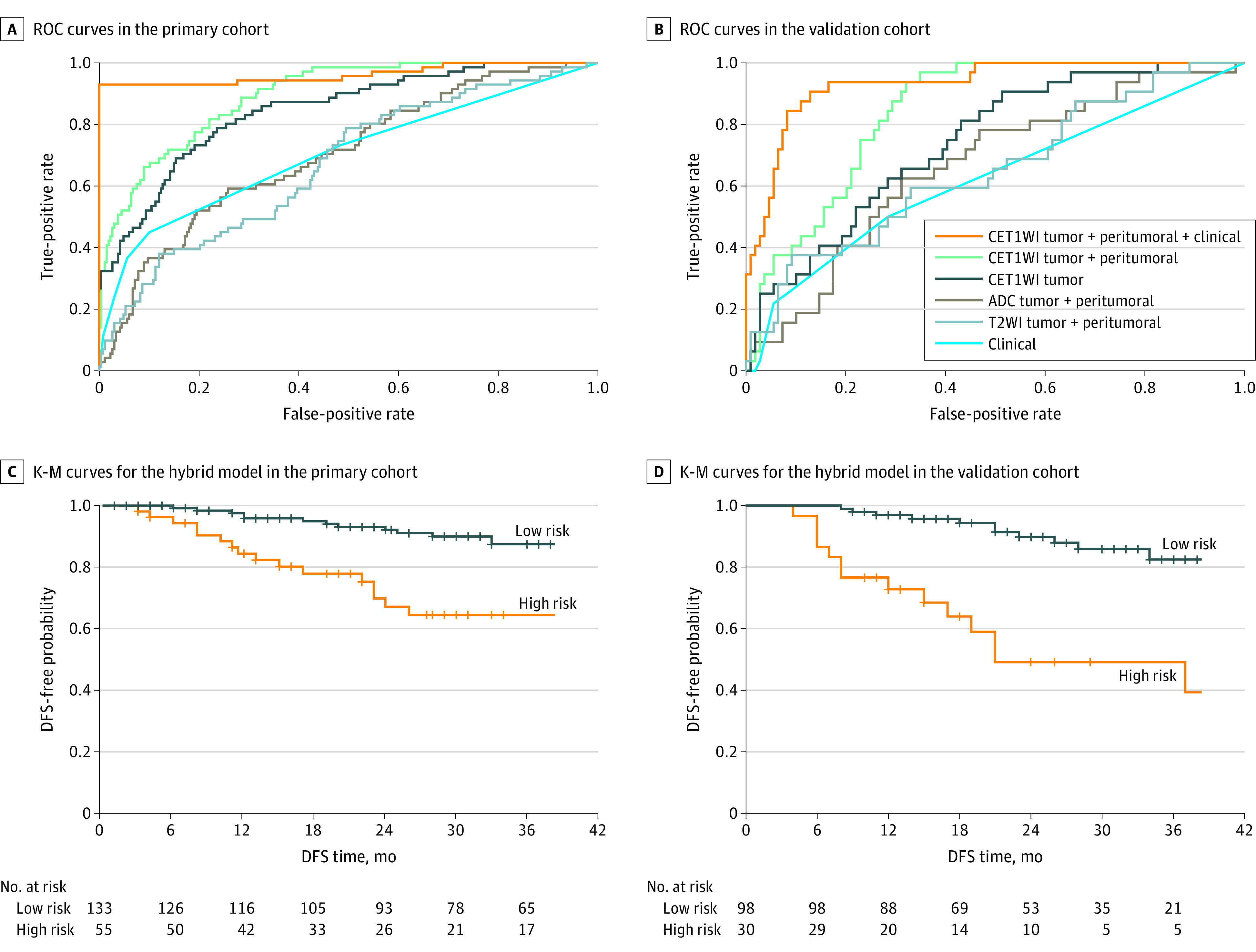
Results: A total of 479 patients (mean [SD] age, 49.1 [9.7] years) fulfilled the eligibility criteria and were enrolled in the primary (n = 338) and validation (n = 141) cohorts. A total of 71 patients (21.0%) in the primary cohort and 32 patients (22.7%) in the validation cohort had lymph node metastais confirmed by lymphadenectomy. Among the 3 image sequences, the deep learning model that used both intratumoral and peritumoral regions on contrast-enhanced T1-weighted imaging showed the best performance (AUC, 0.844; 95% CI, 0.780-0.907). These results were further improved in a hybrid model that combined tumor image information mined by deep learning model and MRI-reported lymph node status (AUC, 0.933; 95% CI, 0.887-0.979). Moreover, the hybrid model was significantly associated with disease-free survival from cervical cancer (hazard ratio, 4.59; 95% CI, 2.04-10.31; P < .001).
Conclusions and relevance: The findings of this study suggest that deep learning can be used as a preoperative noninvasive tool to diagnose lymph node metastasis in cervical cancer.
Conflict of interest statement
Figures
Similar articles
-
Ranking attention multiple instance learning for lymph node metastasis prediction on multicenter cervical cancer MRI.J Appl Clin Med Phys. 2024 Dec;25(12):e14547. doi: 10.1002/acm2.14547. Epub 2024 Oct 6. J Appl Clin Med Phys. 2024. PMID: 39369718 Free PMC article.
-
Magnetic resonance imaging radiomics predicts preoperative axillary lymph node metastasis to support surgical decisions and is associated with tumor microenvironment in invasive breast cancer: A machine learning, multicenter study.EBioMedicine. 2021 Jul;69:103460. doi: 10.1016/j.ebiom.2021.103460. Epub 2021 Jul 4. EBioMedicine. 2021. PMID: 34233259 Free PMC article. Clinical Trial.
-
Development and Validation of a Preoperative Magnetic Resonance Imaging Radiomics-Based Signature to Predict Axillary Lymph Node Metastasis and Disease-Free Survival in Patients With Early-Stage Breast Cancer.JAMA Netw Open. 2020 Dec 1;3(12):e2028086. doi: 10.1001/jamanetworkopen.2020.28086. JAMA Netw Open. 2020. PMID: 33289845 Free PMC article.
-
Prediction of Cervical Cancer Lymph Node Metastasis via a Multimodal Transfer Learning Approach.Br J Hosp Med (Lond). 2024 Oct 30;85(10):1-14. doi: 10.12968/hmed.2024.0428. Epub 2024 Oct 29. Br J Hosp Med (Lond). 2024. PMID: 39475034 Review.
-
Safety of ovarian preservation in women with stage I and II cervical adenocarcinoma: a retrospective study and meta-analysis.Am J Obstet Gynecol. 2016 Oct;215(4):460.e1-460.e13. doi: 10.1016/j.ajog.2016.04.023. Epub 2016 Apr 29. Am J Obstet Gynecol. 2016. PMID: 27133009 Review.
Cited by
-
The pathological risk score: A new deep learning-based signature for predicting survival in cervical cancer.Cancer Med. 2023 Jan;12(2):1051-1063. doi: 10.1002/cam4.4953. Epub 2022 Jun 28. Cancer Med. 2023. PMID: 35762423 Free PMC article.
-
Radiomics-based T-staging of hollow organ cancers.Front Oncol. 2023 Aug 30;13:1191519. doi: 10.3389/fonc.2023.1191519. eCollection 2023. Front Oncol. 2023. PMID: 37719013 Free PMC article. Review.
-
What benefit can be obtained from magnetic resonance imaging diagnosis with artificial intelligence in prostate cancer compared with clinical assessments?Mil Med Res. 2023 Jun 26;10(1):29. doi: 10.1186/s40779-023-00464-w. Mil Med Res. 2023. PMID: 37357263 Free PMC article. Review.
-
Ranking attention multiple instance learning for lymph node metastasis prediction on multicenter cervical cancer MRI.J Appl Clin Med Phys. 2024 Dec;25(12):e14547. doi: 10.1002/acm2.14547. Epub 2024 Oct 6. J Appl Clin Med Phys. 2024. PMID: 39369718 Free PMC article.
-
The efficacy of deep learning models in the diagnosis of endometrial cancer using MRI: a comparison with radiologists.BMC Med Imaging. 2022 Apr 30;22(1):80. doi: 10.1186/s12880-022-00808-3. BMC Med Imaging. 2022. PMID: 35501705 Free PMC article.
