

Detection profile of SARS-CoV-2 using RT-PCR in different types of clinical specimens: A systematic review and meta-analysis
- PMID: 32706393
- PMCID: PMC7404904
- DOI: 10.1002/jmv.26349
Detection profile of SARS-CoV-2 using RT-PCR in different types of clinical specimens: A systematic review and meta-analysis
Abstract
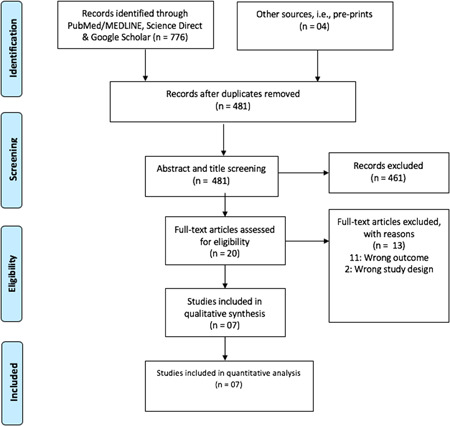
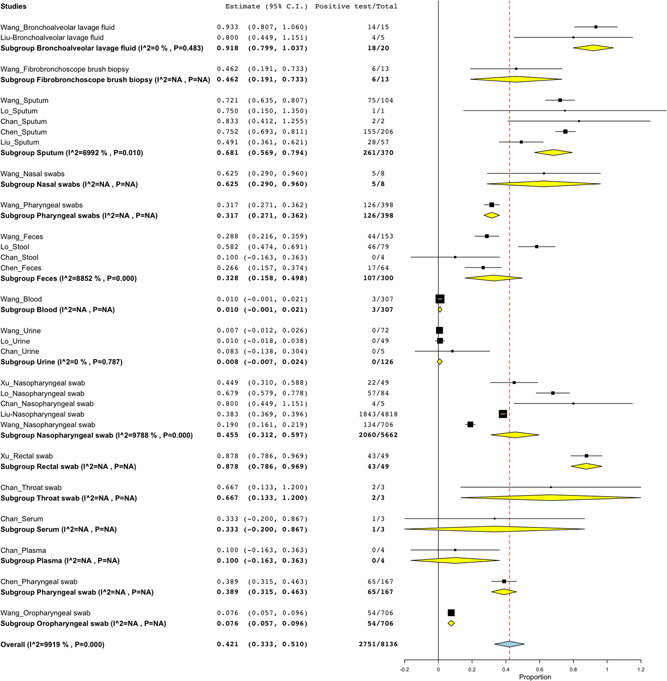
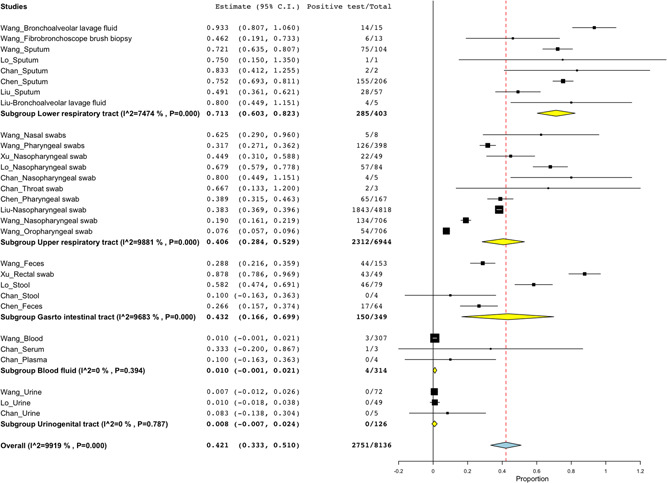
Testing is one of the commendable measures for curbing the spread of coronavirus disease (COVID-19). But, it should be done using the most appropriate specimen and an accurate diagnostic test such as real-time reverse transcription-polymerase chain reaction (qRT-PCR). Therefore, a systematic review was conducted to determine the positive detection rate of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in different clinical specimens using qRT-PCR. A total of 8136 pooled clinical specimens were analyzed to detect SARS-CoV-2, the majority were nasopharyngeal swabs (69.6%). A lower respiratory tract (LRT) specimens had a positive rate (PR) of 71.3% (95% confidence interval [CI]: 60.3%-82.3%) while no virus was detected in the urinogenital specimens. Bronchoalveolar lavage fluid (BLF) specimen had the PR of 91.8% (95% CI: 79.9%-103.7%), followed by rectal swabs; 87.8% (95% CI: 78.6%-96.9%) then sputum; 68.1% (95% CI: 56.9%-79.4%). A low PR was observed in oropharyngeal swabs; 7.6% (95% CI: 5.7%-9.6%) and blood samples; 1.0% (95% CI: -0.1%-2.1%) whereas no SARS-CoV-2 was detected in urine samples. Feces had a PR of 32.8% (95% CI:1 5.8%-49.8%). Nasopharyngeal swab, a widely used specimen had a PR of 45.5% (95% CI: 31.2%-59.7%). In this study, SARS-CoV-2 was highly detected in LRT specimens while no virus was detected in urinogenital specimens. BLF had the highest PR followed by rectal swab then sputum. Nasopharyngeal swab which is widely used had moderate PR. Low PR was recorded in oropharyngeal swab and blood samples while no virus was found in urine samples. Last, the virus was detected in feces, suggesting SARS-CoV-2 transmission by the fecal route.
Keywords: COVID-19; SARS-CoV-2; clinical sample; clinical specimen; polymerase chain reaction.
© 2020 Wiley Periodicals LLC.
Conflict of interest statement
The authors declare that there are no conflict of interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
