

Novel Stepped Care Approach to Provide Education and Exercise Therapy for Patellofemoral Pain: Feasibility Study
- PMID: 32706674
- PMCID: PMC7407256
- DOI: 10.2196/18584
Novel Stepped Care Approach to Provide Education and Exercise Therapy for Patellofemoral Pain: Feasibility Study
Abstract
Background: Patellofemoral pain (PFP) impairs joint- and health-related quality of life and may be associated with knee osteoarthritis. We developed a novel, 2-phase, stepped-care approach for PFP, combining (1) self-directed web-based education and exercise therapy with (2) physiotherapist-supported education and exercise therapy. Physiotherapy sessions can be provided using 2 different modalities: face-to-face and telerehabilitation.
Objective: This study aims to (1) determine the feasibility of our stepped-care approach, (2) explore patient-reported outcomes following self-directed web-based education and exercise therapy in people with PFP (phase 1), and (3) estimate the differences in treatment effects between face-to-face and telerehabilitation to support further education and exercise therapy (phase 2) in those who had not completely recovered following self-directed care.
Methods: Phase 1 involved 6 weeks of self-directed web-based education and exercise therapy. Phase 2 involved random allocation to a further 12 weeks of physiotherapist-led (up to 8 sessions) education and exercise therapy delivered face-to-face or via telerehabilitation to participants who did not rate themselves as completely recovered following phase 1. Feasibility indicators of process, adherence, and participant retention were collected as primary outcomes alongside patient-reported outcomes on Global Rating of Change and knee pain, disability, knee-related quality of life, pain catastrophism, kinesiophobia, and knee self-efficacy. All participants were assessed at baseline, 6 weeks, and 18 weeks.
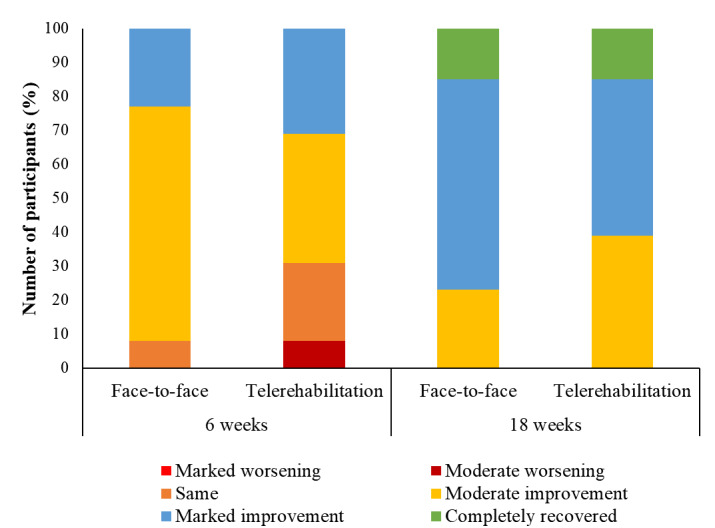
Results: A total of 71 participants were screened to identify 35 participants with PFP to enter the study. Overall, 100% (35/35) and 88% (31/35) of the participants were followed up with at 6 and 18 weeks, respectively. In phase 1 of the study, participants accessed the My Knee Cap website for an average of 6 (7.5) days and performed the exercises for an average of 2.5 (3.6) times per week. A total of 20% (7/35) of the participants reported that they had completely recovered at 6 weeks. Furthermore, 93% (26/28) of the participants who were followed up and had not completely recovered at 6 weeks agreed to be enrolled in phase 2. No statistically significant differences were found between the face-to-face and telerehabilitation groups for any outcome. The novel stepped-care approach was associated with marked improvement or complete recovery in 40% (14/35) of the participants following phase 1 and 71% (25/35) of the participants following phase 2.
Conclusions: Self-directed web-based education and exercise therapy for people with PFP is feasible, as noted by the high rate of participant retention and home exercise adherence achieved in this study. Furthermore, 20% (7/35) of people reported complete recovery at 6 weeks. Both face-to-face and telerehabilitation physiotherapy should be considered for those continuing to seek care, as there is no difference in outcomes between these delivery modes. Determining the efficacy of the stepped-care model may help guide more efficient health care for PFP.
Keywords: eHealth; internet; knee; pain; rehabilitation.
©Danilo De Oliveira Silva, Marcella F Pazzinatto, Kay M Crossley, Fabio M Azevedo, Christian J Barton. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 22.07.2020.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures

References
-
- Smith BE, Selfe J, Thacker D, Hendrick P, Bateman M, Moffatt F, Rathleff MS, Smith TO, Logan P. Incidence and prevalence of patellofemoral pain: a systematic review and meta-analysis. PLoS One. 2018;13(1):e0190892. doi: 10.1371/journal.pone.0190892. http://dx.plos.org/10.1371/journal.pone.0190892 - DOI - DOI - PMC - PubMed
-
- Crossley KM, Stefanik JJ, Selfe J, Collins NJ, Davis IS, Powers CM, McConnell J, Vicenzino B, Bazett-Jones DM, Esculier J, Morrissey D, Callaghan MJ. 2016 patellofemoral pain consensus statement from the 4th international patellofemoral pain research retreat, Manchester. Part 1: Terminology, definitions, clinical examination, natural history, patellofemoral osteoarthritis and patient-reported outcome measures. Br J Sports Med. 2016 Jul;50(14):839–43. doi: 10.1136/bjsports-2016-096384. http://bjsm.bmj.com/cgi/pmidlookup?view=long&pmid=27343241 - DOI - PMC - PubMed
-
- Briani RV, Pazzinatto MF, De Oliveira Silva D, Azevedo FM. Different pain responses to distinct levels of physical activity in women with patellofemoral pain. Braz J Phys Ther. 2017;21(2):138–43. doi: 10.1016/j.bjpt.2017.03.009. http://europepmc.org/abstract/MED/28460712 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
