

The evolution of interventional oncology in the 21st century
- PMID: 32706978
- PMCID: PMC7465871
- DOI: 10.1259/bjr.20200112
The evolution of interventional oncology in the 21st century
Abstract
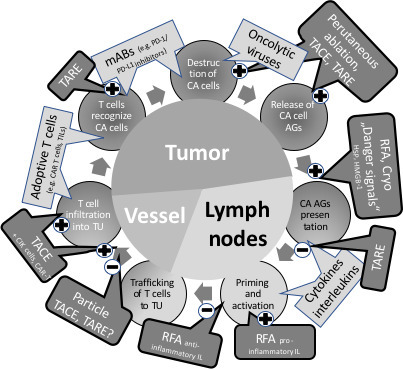
Interventional oncology (IO) has proven to be highly efficient in the local therapy of numerous malignant tumors in addition to surgery, chemotherapy, and radiotherapy. Due to the advent of immune-oncology with the possibility of tumor control at the molecular and cellular levels, a system change is currently emerging. This will significantly rule oncology in the coming decades. Therefore, one cannot think about IO in the 21st century without considering immunology. For IO, this means paying much more attention to the immunomodulatory effects of the interventional techniques, which have so far been neglected, and to explore the synergistic possibilities with immuno-oncology. It can be expected that the combined use of IO and immuno-oncology will help to overcome the limitations of the latter, such as limited local effects and a high rate of side-effects. To do this, however, sectoral boundaries must be removed and interdisciplinary research efforts must be strengthened. In case of success, IO will face an exciting future.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
