

Normal pulmonary venous anatomy and non-anomalous variations demonstrated on CT angiography: what the radiologist needs to know?
- PMID: 32706997
- PMCID: PMC7715996
- DOI: 10.1259/bjr.20200595
Normal pulmonary venous anatomy and non-anomalous variations demonstrated on CT angiography: what the radiologist needs to know?
Abstract
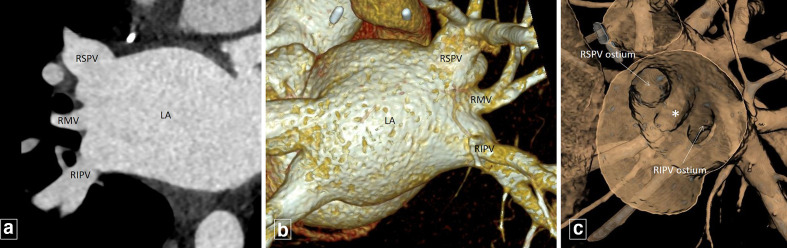
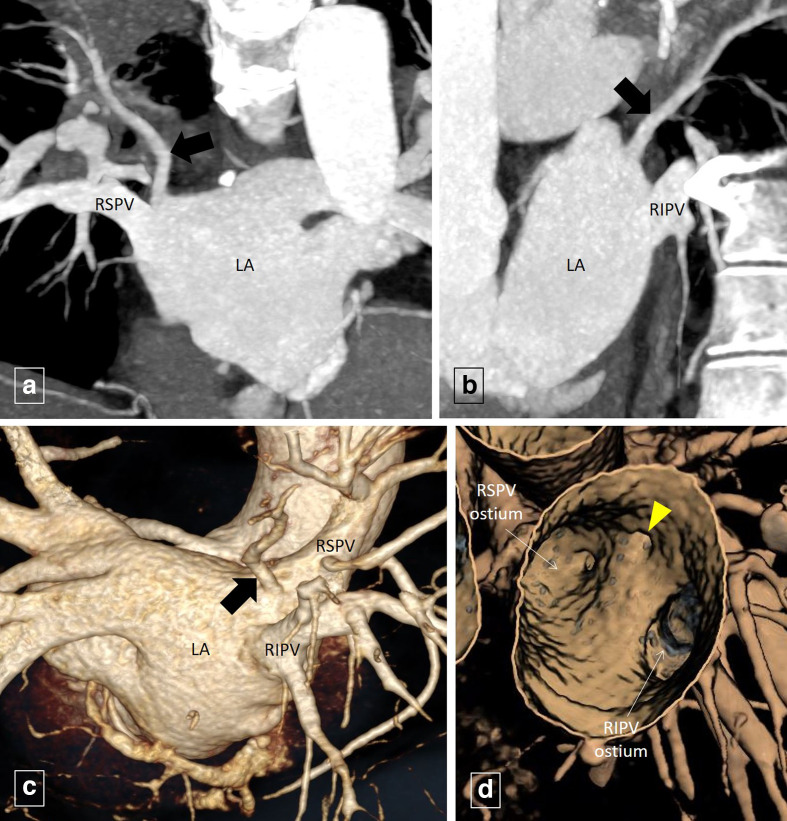
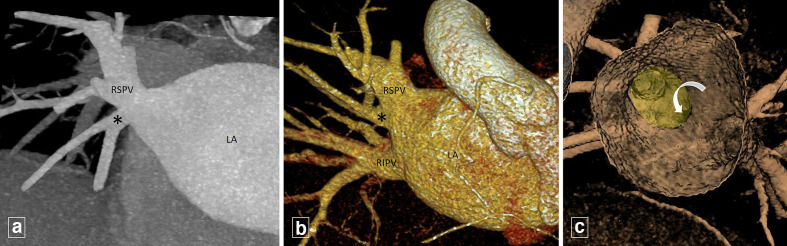
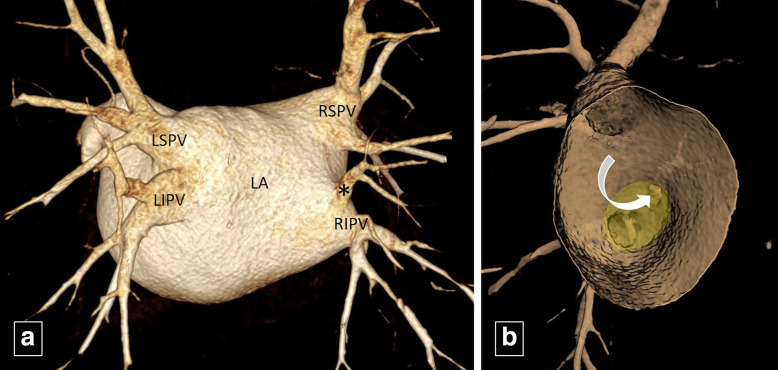
Variations in pulmonary venous anatomy (in the absence of any anomalous pulmonary venous connections) is not uncommon. Commonly occurring variations include presence of conjoined pulmonary veins (PV), supernumerary PVs and ostial PVs. Variant PV anatomy is often asymptomatic; however, it may assume importance in the pre-procedural planning prior to cardiothoracic surgeries and radiofrequency catheter-directed ablation for PV isolation. It is therefore important that the radiologist is aware of the conventional normal and variant PV anatomy in addition to obvious abnormalities like anomalous PV drainage or PV stenosis/ occlusion. Multidetector CT (MDCT) is often used as the first-line imaging modality for pre-procedural PV mapping as it provides high quality images with short acquisition times and availability of numerous post-processing tools.This pictorial review focusses on the MDCT-based PV imaging describing the reporting nomenclature, the conventional normal as well as non-anomalous variant PV anatomy along with their clinical significance.
Figures
References
-
- Lacomis JM, Wigginton W, Fuhrman C, Schwartzman D, Armfield DR, Pealer KM. Multi-detector row CT of the left atrium and pulmonary veins before radio-frequency catheter ablation for atrial fibrillation. Radiographics 2003; 23 Spec No : S35–48Oct;23 Spec No:S35-48; discussion. doi: 10.1148/rg.23si035508 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
